Publication scheme - information about the Trust
This 2024/25 annual report contains detailed and important information about the performance and progress of CNTW against our ‘With you in Mind’ strategy. I suspect that many readers will not have the opportunity to read and digest all of the detail, however I hope that those that do find it both informative and useful. I am going to use my introduction to unashamedly pay tribute, recognise and thank some very important people who ensure that CNTW can continue to provide vital services to our communities.
Firstly, I would like to say a huge thank you to our service users, their families and carers for trust they place in CNTW. Secondly, I would like to thank and pay tribute to all of our staff, our volunteers and to statutory and voluntary sector partner organisations for their dedication, professionalism and skilled care. Thirdly, I would like to recognise and thank our Governors for their time and commitment, and my Board Colleagues for their support and guidance. Together you are amazing, and you deserve both recognition and thanks for what you do together!
During this period, I have witnessed how the Board of Directors has worked diligently to oversee the strategic direction and delivery of the organisation, manage risk and steer our culture and values. This has been in line with our strategy, ‘With You in Mind’. The Board has overseen and approved a number of enabling strategies during the year, which further set out our strategic priorities in specific areas to help achieve our overall ambitions, some of which include quality of care, workforce, digital services and estates. The overriding theme of our Board discussions has been to ensure we seek to maximise the benefits of our services for patients across our entire geography to help them recover and be well. We
have and continue to build, develop and deliver services with the people that we serve.
It is without doubt that CNTW has and continues to face numerous operational pressures, particularly in some areas our waiting lists remain much longer than we would like. We recognise that waiting times can be a huge source of frustration, worry and anxiety for those that we serve. Alongside our system partners we will continue to remain focused on dealing with waiting times. It is pleasing to see that through some sustained joint working we now have trajectories that should see some improved performance during 2025/26 and beyond. It is also pleasing to see some improvements in other areas of our performance.
The NHS continues to face significant financial pressures, in that regard CNTW is no different. We have more savings to find in coming years; however, in 2024/25 intense work was undertaken across the Trust that ensured we finished the year with a positive, balanced budget. We have been recognised by our system partners for our responses to the ongoing financial challenges.
We continue to play a key role in the healthcare system and more than ever this year, we have worked as a collective with other NHS Trusts, our local government partners and the Integrated Care System to share best practices and find new and innovative solutions to meet common challenges and achieve our shared ambitions. With many services and facilities available to our service users and carers across the footprint of the Trust, this partnership working benefits us all.
Once again, I have been so impressed by the commitment of our colleagues. The progress we have made despite the pressures and resource constraints has been down to each and every individual in our organisation pulling together to do what’s best for our patients and local communities.
I have been struck by the invaluable support from our volunteers. Many people give their time in different ways across our services to enhance patient experience. Our Governors make a particularly valuable contribution by representing their communities and each commits real energy and expertise to our ongoing work.
As we look ahead to 2025/2026, we do so with optimism and determination but never complacency. We have laid strong foundations that we can build upon in the coming years. We will seek to further improve our performance, achieve higher quality and work towards a financially sustainable future.
I sincerely hope every single person working with and for CNTW feels positive about what they have individually and collectively achieved this year – you definitely should because you do amazing things every single day!
Thank you!
![]()
Darren Best
Chair
25 June 2025
Welcome to our annual report and accounts 2024/25. This report looks at the last 12 months, talks about progress we have made, and the challenges faced, and describes our priorities for 2025/26. Our strategy ‘With you in Mind’ sets out how we will create a simpler more joined up system of care across CNTW, working with partners and building a rights based, trauma-informed, human and compassionate approach. It sets out how we will build a joined up, lifelong, continuous model of care and support, with the focus on responding well to people's needs early, looking to avoid crisis wherever possible, but
recognising that when people reach crisis, we respond quickly and well.
Through this year we have further progressed work on our Model of Care and Support. At its heart is a partnership across primary care, secondary mental health NHS services, the Voluntary, Charitable and Social Enterprise Sector and Local Authorities, working alongside local communities. Our aim is to enable people easy access to help when they need it, to build up continuous relationships that enable us to respond well and quickly to people’s changing needs, and to ensure that when people need more specialist help, treatment or support, it is provided by the right people when it is needed. The principles of our model of care and support apply across everything we do – they are grounded in humanity, respect for rights, partnership, continuity and fostering effective long-term relationships. We are going further and faster with this model in Whitehaven in West Cumbria, where we are a national pilot for new models of community care. But the model is our guide for the development of our model across the whole of the Trust
It is important that we take practical steps and ensure that we provide safe and effective care every day. We have set clear quality priorities for the year and have made significant progress. We have introduced a new approach to learning from incidents, grounded in a just and learning culture, and have significantly reduced our use of restrictive practice. We have progressed work on the triangle of care, working to ensure that as professionals we work in partnership with people, their carers and families to get care right on an individual basis and across the organisation. We want to be an organisation that co-creates – that
really values the views of the people and communities that we serve. We want to take the next steps in service user and carer involvement, so that it is deeply embedded in everything we do and in every decision that we make. And we have made further progress in embedding research and innovation across our organisation, as one of the most research active organisations of our type in the country. The detail of our delivery against our quality priorities is included in our Quality Account.
We have delivered against our financial goals for the year, in a year that was hugely pressured across the whole of the NHS. After a year of significant challenge, we made a small surplus. This is turn has enabled us to maintain our cash balances and pay off our long-term debts associated with the redevelopment of our estate over the years. We have largely completed our CEDAR scheme (Care, Environment, Development, and Reprovision), which is a nationally backed programme to re-provide our inpatient secure services, our adults acute inpatient services for Newcastle and to improve our wards
supporting Children and Young People at Ferndene. We will deliver this significant scheme
within budget.
We continue to be challenged with the length of time that people are waiting to receive care and support, and the demand and pressures on our services. This is felt most strongly in our services for children and young people and especially where people are asking for an assessment for ADHD or autism. Our in-patient services continue to be busy and often challenging places to work and managing demand for our services and responding to people well when they need us requires continuous effort and focus.
We have received a challenging draft CQC report regarding our inpatient services for people with learning disabilities and autism, which continues to be described a requiring improvement. While we await the final report, we have learned from and welcome the draft and have put in place a wide range of actions to respond to the CQCs concerns. We continue to see our regulators as positive contributors to enable us to reflect on that care that we provide and how we can improve it.
On behalf of everyone at Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, I would like to extend my thanks to our members, governors, service user and carers and staff for your commitment and support over the past 12 months. When I reflect on our Trust and acknowledge the inspirational desire to continuously improve services for service users, carers and staff, I am struck by the commitment to teamwork and collective effort. This year, we will continue to improve together. I hope you enjoy reading the annual report and agree that we have had a challenging but successful year.
![]()
James Duncan
Chief Executive
25 June 2025
1.1 Overview of Performance
This report has been prepared on a ‘group’ basis and will refer to Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust Group as ‘CNTW’ or ‘the Group’. The CNTW ‘group’ includes NTW Solutions Limited, our wholly owned subsidiary company.
Sections of this report that is relevant to the NHS services provided by Cumbria,
Northumberland, Tyne and Wear NHS Foundation Trust will be referred to as ‘the Trust’.
Northumberland, Tyne and Wear NHS Foundation Trust will be referred to as ‘the Trust’.
This overview will provide an understanding of the CNTW Group, including the services we
provide, our organisational vision and values, strategic direction, and potential risks as well
as a summary of our performance during 2024/2025.
Going Concern Disclosure
After making enquiries, the directors have a reasonable expectation that the services provided by the NHS Foundation Trust will continue to be provided by the public sector for the foreseeable future. For this reason, the directors have adopted the going concern basis in preparing the accounts, following the definition of going concern in the public sector adopted by HM Treasury’s Financial Reporting Manual.
After making enquiries, the directors have a reasonable expectation that the services provided by the NHS Foundation Trust will continue to be provided by the public sector for the foreseeable future. For this reason, the directors have adopted the going concern basis in preparing the accounts, following the definition of going concern in the public sector adopted by HM Treasury’s Financial Reporting Manual.
Our History
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust (CNTW) was formed on 1 October 2019 following the transfer of mental health and learning disability services from Cumbria Partnership NHS Foundation Trust to Northumberland, Tyne and Wear NHS Foundation Trust. Northumberland, Tyne and Wear NHS Trust was established on 1 April 2006 following the merger of three Trusts: Newcastle, North Tyneside and Northumberland Mental Health NHS Trust, South of Tyne and Wearside Mental Health NHS Trust and Northgate and Prudhoe NHS Trust. The Trust achieved authorisation as an NHS Foundation Trust on 1 December 2009. As a Public Benefit Corporation CNTW has members. We have four membership constituencies to represent stakeholder interests:
• Public constituency
• Service users and carers constituency
• Staff constituency
• Partner organisation constituency.
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust (CNTW) was formed on 1 October 2019 following the transfer of mental health and learning disability services from Cumbria Partnership NHS Foundation Trust to Northumberland, Tyne and Wear NHS Foundation Trust. Northumberland, Tyne and Wear NHS Trust was established on 1 April 2006 following the merger of three Trusts: Newcastle, North Tyneside and Northumberland Mental Health NHS Trust, South of Tyne and Wearside Mental Health NHS Trust and Northgate and Prudhoe NHS Trust. The Trust achieved authorisation as an NHS Foundation Trust on 1 December 2009. As a Public Benefit Corporation CNTW has members. We have four membership constituencies to represent stakeholder interests:
• Public constituency
• Service users and carers constituency
• Staff constituency
• Partner organisation constituency.
Our Services
CNTW provides a wide range of mental health, learning disability, Autism and neurorehabilitation services to a population of 1.7 million people across North Cumbria and the North East of England as well as providing specialist services nationally. We are one of the largest mental health and disability organisations in the country. We employ over 9,000 staff, operate from over 70 sites and provide a range of services including many regional and national services. The Trust has an annual turnover of around £647 million.
We support people in the communities of North Cumbria, Northumberland, Newcastle, North Tyneside, Gateshead, South Tyneside and Sunderland working with a range of partners to deliver care and support to people in their own homes and from community and hospital-based premises. Our main hospital sites are:
• Carleton Clinic, Carlisle
• Walkergate Park, Newcastle upon Tyne;
• St. Nicholas Hospital, Newcastle upon Tyne;
• St. George’s Park, Morpeth;
• Northgate Hospital, Morpeth;
• Hopewood Park, Sunderland;
• Monkwearmouth Hospital, Sunderland; and
• Ferndene, Prudhoe.
Cumbria, Northumberland Tyne and Wear NHS Foundation Trust at a glance

Chief Executive’s Statement on the Performance of the Trust
Despite the challenges over the past 12 months, the Trust has continued to move forward with the major change programmes of work which significantly underpin our strategic ambitions.
Trust Transformation Programme, supporting and enabling system working, and the
Trust Strategy and Model of Care
In 2023, CNTW launched its Strategy With you in Mind for the future to work together, with compassion and care, to keep you well over the whole of your life. The strategy sets out five strategic ambitions to deliver the goals and changes we want to see across our services both now and in the future. Underpinning our ability to deliver the Trusts strategic ambitions is the ability to deliver our Model of Care and Support which launched in 2024.
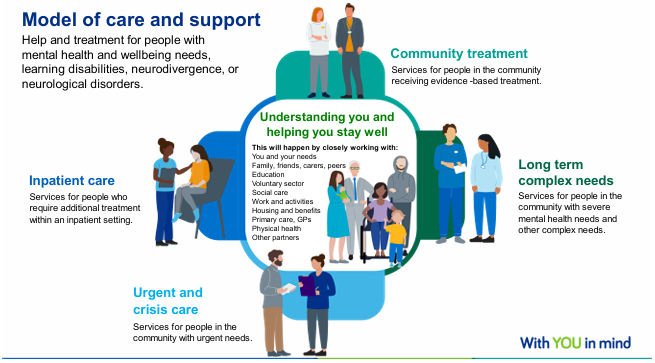
The key areas of transformation are managed by a single Transformation Board with subgroups linked to the Model of Care above. This will ensure our improvement focus is linked to our Strategy and Model of Care. Transformation Board subgroups are based on the five elements of the Model of Care and Support:
• Understanding you and helping you stay well
• Community Treatment
• Long term complex needs
• Urgent and crisis care
• Inpatient care
These groups focus on core transformation areas where the Trust is implementing national guidance and working with the ICB and wider system.
The latest national guidance on community transformation in mental health is aligned with the new government's neighbourhood health service models. The Trust has long been working to the national guidance on community transformation in mental health which emphasises a whole-person, whole-population approach, with the aim of developing integrated models of primary and community mental health care. This includes access to psychological therapies, improved physical health care, employment support, Housing and benefits support, personalised and trauma-informed care, and support for self-harm and coexisting substance use.
The Trust has also been working to the Long-Term Plan national guidance on mental health and urgent and crisis needs, focusing on ensuring timely and appropriate care for individuals experiencing a mental health crisis. The NHS Long Term Plan emphasises the importance of providing comprehensive crisis pathways in every area, which can be accessed through communities, homes, emergency departments, inpatient services, or even ambulance transport and now 111 press Mental Health. The goal is to offer a range of crisis services, including crisis resolution home treatment, liaison mental health services, and alternative models like crisis cafes and safe havens. This approach aims to improve access, experience and outcomes for those in urgent need of mental health support.
The National Mental Health Inpatient Quality Transformation Programme and the Commissioning Framework for Mental Health Services emphasise the local provision of high-quality mental health care within communities. In line with this, the Trust has prioritised key aspects of the programme, including appropriate admissions, the delivery of therapeutic care, and effective discharge planning. In July 2024, the North East and North Cumbria Integrated Care Board (ICB) produced their Mental Health, Learning Disability and Autism Inpatient Quality Transformation Plan in response to the national framework for inpatient quality transformation. The Trust is supporting this, working with partners across the system.
Communities and organisations will collaborate more effectively to address needs, reduce repeated referrals, and help people maintain their wellbeing. The goal is to harness the strengths of individuals and their communities to improve secondary prevention and prevent wellbeing from deteriorating to the point of requiring secondary mental health services. By combining community assets and resources, patients, carers, and families can support individuals to stay well and gain a deeper understanding of the
holistic mental health and wellbeing needs within our communities.
This approach removes traditional team and service boundaries, tailoring support to each person’s needs and priorities while recognising risk, choice, and ownership. The aim is to connect individuals with their communities to achieve better mental health, wellbeing, and active citizenship.
This neighbourhood health service approach (Neighbourhood Health Service models) focuses on bringing care closer to people’s homes, making it easier to access and ensure that health and all other partners working in the community work smoothly together. This is especially important as more people face complex health problems and spend a greater part of their lives dealing with illness. The aim is to create healthier communities, helping people of all ages to live active, independent lives for as long as
possible.
Instead of different parts of the health system working separately, leading to delays, repeated efforts, and frustration for patients and staff, this approach encourages everyone involved in supporting people in communities with their health and wellbeing, to work as a team. Some areas are already making progress with this way of working, and guidelines are being provided to help others build on this, adapting the plans to fit their local needs. The Hope Haven in West Cumbria is nationally one of six 24/7
neighbourhood mental health centres to support the transformation in joined up person centred mental health and wellbeing care.
By better connecting services, using resources wisely, and giving people more control over their own care, neighbourhood health strives to improve the experience and outcomes for everyone.
People receiving support in the 'understanding you and helping you stay well' section of the model may also need care from secondary care services which sit around the central part of the model and only to be used when really needed. The Trust will play a supportive role in the 'understanding you and helping you stay well' section, while taking the lead in the secondary care focused areas of the model. Regardless of whether someone is an inpatient, in crisis, or receiving community support, the role of local communities remains essential. Local wellbeing support must always be at the heart of an individual’s care and
support.
Community Treatment
People will have quicker access to evidence based treatments and interventions to meet their mental health needs including for both psychosis and non psychosis.
The community treatment aspect of the care and support model is designed to provide targeted and timely support to individuals. It will focus on delivering episodic treatment, regular monitoring, and brief interventions to address immediate needs effectively.
Where further assessment is required, it will facilitate referrals to specialist pathways and the development of tailored treatment plans. The model also aims to expand access to a wide range of specialist community treatments and interventions, ensuring individuals can receive appropriate care closer to home. Close collaboration with the local community team will be a key feature to ensure continuity of care and ensure care is trauma informed.
This will provide clear oversight of care and the ability to integrate additional treatments as needed. Moreover, the delivery of evidence based psychological therapies will be enhanced, ensuring individuals receive high quality mental health support rooted in proven practices. Together, these elements aim to create a responsive, connected, and person centred approach to community care.
The Trust are increasing the provision of treatments to support patients to live in their communities. This includes for example increasing the use of Clozapine as a drug treatment for those with treatment resistant schizophrenia and enhancing systems to support managing this in the community.
The Trust will also reduce reliance on medication for people with learning disabilities and/or autism and proved alternative trauma informed psychosocial approaches. We will create better rehabilitation pathways across community, housing, and inpatient settings. This will be in collaboration with social care and our voluntary sector partners. There will also be a shift away from the Care Programme Approach, developing an integrated approach for this with local authorities and voluntary sector partners. This will allow a shared approach to care planning and risk management in the community.
Long term complex needs
The long term complex needs part of the Model of Care and Support will focus on providing sustained and assertive management for individuals with severe and enduring mental illness and other complex needs, shifting away from episodic care to ensure consistent support.
The Trust clinical team will deliver long term care for those with chronic mental health conditions, supported by assertive and intensive case management through the Community Treatment Teams. A particular focus will be placed on the cohort of patients with the most needs, with tailored monitoring and intervention plans designed to stabilise their conditions and prevent further deterioration. Support will be provided for as long as it is needed, with a dedicated key worker assigned to each individual to ensure continuity of care.
Families and carers will play an essential role as active partners in this process. The approach aims to improve outcomes for this group, reducing the percentage of patients with severe mental illness (SMI) who experience deterioration or require crisis services, as well as lowering readmission rates and Community Treatment Order recalls. Innovation in this area is being prioritised in line with emerging national guidance, including the adoption of new treatments for people with severe mental illnesses, along with enhanced physical health care, all with the overarching goal of fostering better health and wellbeing for this population.
Urgent and crisis care
We will improve access to urgent care and work with our partners to support people with effective safety planning, identify deterioration quickly and provide access to crisis support and interventions.
We will provide seamless, responsive support for individuals during times of acute need by fostering greater alignment and integrated working between both across the pathway of care within the Trust and with our communities and partners. It prioritises needs based clinical decision making at the interface with inpatient care and emphasises the prevention of deterioration through effective collaboration with community services. Crisis support will focus on offering alternatives to 11 hospital admission, working closely across a patient’s pathway to deliver solutions that reduce the need for repeat assessments and ensure care continuity through a single triage approach.
This part of the model seeks to decrease the number of new, repeat, or frequent crisis attenders, minimise emergency Department visits to an Acute Hospital, reducing waiting times, and reducing self harm and suicide rates. Efforts will also aim to improve readmission rates, enhance home based treatments, and ensure services are tailored to support individuals with Autism, Learning Disabilities, and complex emotional needs. Overall, the approach is designed to provide compassionate, efficient, and person centred crisis care that improves outcomes and supports recovery.
Inpatient care
The inpatient care part of the model focuses on providing purposeful, therapeutic, and person centred care while protecting people’s human rights and ensuring a welcoming, healing environment on wards. People will only be admitted when hospital level care is necessary, with a clear purpose for the stay. Therapeutic care is carefully planned and reviewed with the individual and their carers, ensuring they receive daily interventions and treatments to support recovery.
From the start of their stay, discharge planning is a priority, making transitions home or to another ward smooth, with post discharge support in place to help people stay well. This supports the regional and national improvement work as part of the wider Inpatient Quality Transformation.
Collaboration with social care, housing providers, GPs, and primary care will ensure ongoing wellbeing after discharge, with services designed to reduce the need for hospital stays. Staff must have the right skills to deliver effective treatment, supported by continuous improvement of care pathways through data, co production, and innovation. The model also emphasises reducing restrictive practices and fostering a culture of respect, aiming for better outcomes, improved patient and staff experiences, and care that priorities recovery, dignity, and community connection.
Construction on our CEDAR scheme will complete in 2025/26. The Sycamore Unit opened in November 2023 and provides state of the art facilities for secure inpatients at our Northgate site. The work on developments for our Children and Young People Services (CYPS) at our Ferndene site completed in March 25 and the building work on the St Nicholas Hospital site to support our Newcastle Inpatient services is scheduled to complete in Summer 2025. The CEDAR scheme was announced in October 2020 as one
of the 40 schemes to be developed under the Health Infrastructure Plan, which commits £3.7bn to deliver 40 hospitals by 2030.
Provider Collaboratives
The Trust continues to work in partnership with Tees, Esk and Wear Valleys NHS FT on commissioning Adult Secure Services, Children and Young People Tier 4 Services and 12 Adult Eating Disorders services. The aim of this partnership is to develop and improve services for the population of North East and North Cumbria, ensuring long term stability in full collaboration with partners, service users and carers. The Trust has worked with the NENC Integrated Care Board and NHS England and commissioning arrangements for the Perinatal service began through the Provider Collaborative, in October 2024. We are also lead provider for OpCourage (veteran’s) provider collaborative working in partnership with four NHS Foundation Trusts and two voluntary sector organisations to provide services for populations across the North East, Yorkshire and the North West.
Supporting and enabling the development of the North East and North Cumbria Integrated Care System
CNTW continues to play a key role in the ongoing development of the North East and North Cumbria Integrated Care System (NENC ICS) which works to deliver significant change in the way health and care services are planned and delivered across our region. We continue to work with system partners including local authorities, voluntary and community sector (VCS) organisations and NHS colleagues to develop innovative approaches to care and support underpinned by meaningful involvement of people with mental health issues and learning disabilities in this work.
As a key partner in the NENC ICS Mental Health, Learning Disabilities and Autism Executive Board over the past year the Trust has supported the delivery of key objectives for the transformation of mental health and learning disability and autism services in our region, much of which is described above. We look forward continuing to work in partnership with colleagues across the system and with people with lived experience of mental illness and learning disabilities over the coming year as our Integrated Care System continues to develop.
Improving care for people with autism and learning disabilities
Accessing care and support can be challenging for patients living with autism and/or learning disabilities and their families and we are committed to working in partnership with people who use our services to improve the way we deliver care as well as our physical environments. Over the past year we have continued to work in collaboration with people with autism to address how we can improve care, treatment, and the ward environment for people with autism who are admitted to our services.
We continue to work with advocacy services across the CNTW footprint to help strengthen the voice of all patients, including those with autism and learning disabilities, within our inpatient units. The Trust continues to work with people with lived experience of autism and community organisations to roll out autism training to Trust staff.
HOPEs is the recommended national model for working with individuals in Long Term Segregation (LTS). Individuals with learning disability and autistic individuals are more likely to be subject to highly restrictive practices such as LTS. The Trust is committed to reducing its use and has invested in a HOPEs role to lead the implementation of the model in CNTW and support the work of the National HOPEs team.
All individuals in the Trust who are in LTS are supported using the model that addresses their human rights and works to improve their quality of life and end LTS. Staff supporting these individuals are being trained in the model and to use a tool to support them in setting intervention targets to change the situation. More information on the impact of the HOPEs model can be found in our Quality Account.
Health and Safety Executive Improvement Notice
In February 2024, the Trust was issued with an improvement notice by the Health and Safety Executive (HSE) which highlighted issues relating to systems and processes to identify and manage incidents and risks associated with violence and aggression. The Trust responded to the HSE that outlined the improvements made to systems, processes and policies to ensure the ongoing effectiveness of managing such incidents across the Trust. This included:
• Strengthening of policies and associated Practice Guidance Notes (PGNs) to enhance reference to risks of violence and aggression toward staff as well as patients.
• Further work and clarity of actions to reduce the risk of violence aggression towards staff including health and safety training.
• Improving engagement with front line staff reflecting personal experiences of violence and aggression and associated learning and risks assessments.
Throughout the year, there has been a reduction in incidents of violence and aggression through monitoring of actions and learning via the Prevention and Management of Violence and Aggression Task and Finish Group. Assurance is provided on an ongoing basis to the Trust Board Quality and Performance Committee, and this continues to be an area of key focus for the Board.
Although there was a recognition there will be incidents of violence and aggression in our services at times there are systems and processes in place to both mitigate the risk of such incidents occurring (in terms of frequency and severity of incidents) and support for staff to manage such incidents. The improvement notice also highlighted the opportunity for the Trust to look at data collected in order to monitor and identify themes which informs the longer term improvements we need to make.
In October 2023, the Trust launched an engagement exercise, open to all staff, on changing the operational structure for the Trust. Following the Trust wide engagement exercise, the new operating structure came into effect in April 2024.
The Trust moved from a structure based on four localities (North, South, Central and North Cumbria), to three operational Care Groups:
• Community Care Group
• Inpatient Care Group
• Specialist Care Group
Community Care Group
The new operating structure has one Community Care Group covering all seven ‘places’ and existing access and community CBUs. Places refers to what was previously known as localities (Newcastle, North Cumbria, North Tyneside, Northumberland, South Tyneside, Gateshead, Sunderland). Integrated Care Systems (ICS) refer to ‘places’ as a geographic footprint which often aligns with a local authority area or patient flows for acute care. This is to allow Trusts across the country to work with partners to provide better joined up care in the places that people live and work.
One of the main drivers in the changes to the structure has been the ability to go further with our transformation of community services at place to deliver the aims of our Model of Care and Support. Strengthening of the leadership roles of the place directors, combined with the Clinical Business Units across community and access will be pivotal in implementing the changes to the Model of Care and support, including achieving real integration at place.
Inpatient Care Group
The new operating structure has one Inpatient Care Group covering all existing inpatient clinical business and will retain the existing locality inpatient clinical business units. The operational delivery, local knowledge and site leadership were critical factors influencing retaining the local leadership across the sites. The creation of a single in-patient group aligns inpatient care with the commissioning and delivery model across the Integrated Care System. It also allows increased focus on standardisation of approach, embedding a consistent approach to therapeutic, person-centred and recovery-focussed care, as set out in our Model of Care and Support.
Specialist Care Group
The new structure has one Specialist Care Group covering all of the provider collaborative commissioned services and specialist services across the Trust. Work took place across many of the support services within the Trust to update various systems such as dashboards, contact cards, RATIO access requests, cost centres, and the Trust’s staff intranet and public website to reflect the new structures.
A full list of services, with descriptions and contact details can be found on our website.
Wholly Owned Subsidiary Company
The Trust established NTW Solutions Limited (NTW Solutions) as a wholly owned subsidiary company and it became operational in April 2017. Wholly owned subsidiary companies are an organisational and governance form that NHS Foundation Trusts can legally establish to manage parts of their organisation. Wholly owned subsidiary companies are separate legal entities. NTW Solutions is part of the “CNTW Group”, sharing the vision and values of the Trust in carrying out its activities, with the Trust holding 100% of the Company’s shares.
NTW Solutions provides the Trust’s estates and facilities management services and a range of other services including workforce recruitment, staff records, procurement, materials management, some financial services, car leasing and other staff benefit schemes, digital dictation, and outpatient pharmacy dispensing. It employed 884 staff (physical number of staff not full-time equivalents) as of 31st March 2025, approximately half of whom were transferred from the Trust to the company under TUPE regulations, thereby protecting their NHS terms and conditions. New company staff appointed since April 2017 are employed on company terms and conditions of service.
AuditOne
AuditOne, is a not-for-profit provider of internal audit, technology risk and counter fraud services which is hosted by CNTW. AuditOne was originally formed from four NHS consortia and delivers independent assurance and advice to public sector clients on a wide range of topics including financial management, governance, major IT programmes, data quality, cost reduction, integrated assurance, and forensic investigations.
CNTW Charity – SHINE
Our charity continues to make a meaningful difference across CNTW by supporting service users, carers, and staff through projects that enhance care, wellbeing, and connection to our communities. Our SHINE Strategy and plan has been developed in line with the Trust’s Strategic Ambitions.
Strategic Ambition 1 – Quality Care, Every Day
During 2024/25, the charity made 63 allocations, supporting a diverse range of initiatives that improve the care experience. Highlights include a £10,000 investment in bikes for a woodland track at Northgate Hospital, enabling outdoor therapy and promoting physical wellbeing. We continue to fund projects that offer ‘little extras’ through our SHINE General Fund, which celebrated its 10th birthday this year.
Strategic Ambition 2 – Person- Led Care, When and Where It’s Needed
We marked World Mental Health Day by supporting awareness events across our communities, ensuring the charity plays a part in reducing stigma and promoting access to help when and where it’s needed. This focus on community and individual impact is at the heart of every project we fund.
Strategic Ambition 3 – A Great Place to Work
The charity has empowered staff-led fundraising more than ever. Over 35 fundraising efforts were supported – from bake sales and sponsored walks of Hadrian’s Wall to name one, to Trust-wide fairs – raising over £26,500. We also launched a Fundraising Volunteer Committee and introduced Microhive, a new scheme enabling staff to donate spare pennies from their monthly salary. The collective work across the Trust to raise funds for the charity has had a significant impact on staff morale within teams and services across the Trust, with many more activities planned for 2025/26.
Strategic Ambition 4 – Sustainable for the Long Term, Innovating Every Day
This year saw the introduction of textile donation points across all Trust sites, offering a sustainable way for people to support the charity. We also expanded our digital reach with new social media channels, and we’re preparing to launch a dedicated charity website, which will make it even easier to donate, get involved, and see the difference every donation makes.
Strategic Ambition 5 – Working With and For Our Communities
Community and corporate partnerships continued to grow. Our first ever Christmas Charity Concert was made possible with support from Starbucks, Marks and Spencer, and Tesco, raising over £1,500. We also welcomed DJ Schak as our new charity patron, helping to raise awareness and reach new audiences. Local supermarkets – including Sainsbury’s, Morrisons, Asda, and Tesco – have continued to champion our work across the region.
Looking Ahead
As we look to the future, we remain committed to growing our reach, supporting more projects that benefit service users, carers and staff, and continuing to strengthen community partnerships. With the recent launch of our social media channels and the upcoming release of our new dedicated charity website, we’re excited to connect with more people than ever before and make it even easier to get involved.
Following an 18-month process to review the Trust’s strategy, we reflected on the significant changes within the health and care sector and the impact of this on CNTW. This included the impact of the cost-of-living increases to those within our local communities, the increasing demand for health and care services, and the need for us to work more closer than ever with our partners and stakeholders, to change how we deliver health and care services across the North East and North Cumbria Integrated Care System.
Following extensive engagement with service users and carers, our workforce, our partners and local communities, our new strategy, With You in Mind’ was launched in Spring 2023.
Our vision is to “work together, with compassion and care, to keep you well over the whole of your life”. This vision remains based on our values of being caring and compassionate, respectful, honest, and transparent.
To develop our strategy, we asked service users, carers, their families, our staff, and partners to describe what matters to them. They asked us to work together, with them in mind, with compassion, humanity, and care. This is at the heart of our strategy.
We have developed long-term commitments which will guide everything we do. Our aim is to deliver on these commitments every day, in every contact.
Our vision, values, strategic ambitions, and commitments are outlined below.
Our vision
To work together, with compassion and care, to keep you well over the whole of your life.
Our values
We are caring and compassionate... because that is how we'd want others to treat those we love.
We are respectful...because everyone is of equal value, is born with equal rights and is entitled to be treated with dignity. We want to protect the rights of future generations and the planet that sustains us all.
We are honest and transparent...because we want to be fair and open, and to help people make informed decisions.
Our strategic ambitions
Quality care, every day...We will aspire to deliver expert, compassionate, person-led care every day, in every team. We will value research and learning.
A great place to work... We want to be a great place to work. We will make sure that our workforce has the right values, skills, diversity and experience to meet the changing needs of our service users and carers.
Person-led care, when and where it is needed... We will work with partners and communities to support the changing needs of people over their whole lives.
Sustainable for the long term, innovating every day... We will be a sustainable, high performing organisation, use our resources well and be digitally enabled. We will be accountable for the money we spend; we will live within our means, and we will work in a way that is kind to the planet.
Working with and for our communities... We will create trusted, long-term partnerships that work well together to help people and communities.
Our commitments
Commitment to our service users:
- Understand me, my story, my strengths, needs and risks. Work with me and others, so I can keep healthy and safe;
- Protect my rights, choices and freedom;
- Respect me and earn my trust by being honest, helpful and explaining things clearly;
- Support me, my family and carers in an effective, joined-up way that considers all my needs; and
- Respond quickly if I am unwell or in crisis, arranging support from people with the right expertise. Make sure I don’t have to keep repeating my story.
Commitment to our families and carers (also known as our ‘Carer Promise’):
- Recognise, value and involve me;
- Work with me to ensure you’re aware of my needs as a carer;
- Listen to me, share information with me, and be honest with me when there is information you can’t share;
- Talk with me about where I can get further help and information, and about what I can expect from you.
Commitment to our staff:
- Respect me for who I am, trust me, value me and treat me fairly;
- Allow me freedom to act, to use my judgement and innovate in line with our shared values;
- Protect my time by making systems and processes as simple as possible so I can deliver the work I aspire to, learn, progress and get a balance between work and home;
- Offer me safe, meaningful work and give me a voice, working as part of a team that includes other professions and services; and
- Support me with compassionate managers who communicate clearly and understand what it’s like to do my job.
Commitment to our partners and communities:
- Explain what to expect from CNTW;
- Help us to fight illness, unfairness and stigma;
- Make sure that organisations talk to each other and put the needs of people before their own. Share responsibility for getting things right;
- Get to know local communities. Respect their wisdom and history;
- Be responsible with public funds;
- Share our buildings, grounds and land; and
- Protect the planet.
NTW Solutions Limited Strategy
NTW Solutions refreshed its strategy in 2024 to build on the firm foundations established since the company was founded. The overall company strategy is to support our partners to deliver better care by:
• Providing high quality services every day
• Being a great and inclusive place to work
• Having a culture of innovation
• Tackling the climate emergency
• Delivering sustainable growth

This year, there was a lot to be proud of at CNTW. Here are just some of the highlights. Despite the significant challenges the NHS is currently facing, there is still much to be proud of. Here are just some of the highlights from the last year.
In April the Trust demonstrated its commitment to the armed forces community by introducing a declaration for staff. This could be as a service reservist, veteran, member of the Cadet Force Adult Volunteers or a family member. By signing the declaration, staff will be eligible for specialist support such as extra help for relatives and staff on mobilisation and access to the Trust’s Armed Forces Association.
In May the Trust launched a new look website hosting its series of mental health self-help guides. The guides are now as accessible to as many people as possible with a triple AAA rating, meaning that it is accessible to all users, including those with disabilities.
With additional accessibility features, the new website features a modern fresh look and feel and has been designed to enhance user experience and accessibility. With one in six of us experiencing mental ill health at some point in our lives, people need information that is clear, accurate, up-to-date and easy to use. Users can have confidence in the knowledge that the guides have been written with the help of NHS professionals, service users and carers. The guides also have brand new features, such as the ability to type into a guide and save their own personalised version. Our range of self-help guides are available here.
In May our staff also put on their hiking boots and walked the length of Hadrian’s Wall to raise money for the Trust’s charity, the SHINE fund. A wide range of staff from six wards (at the Carlton Clinic in Carlisle and West Cumberland Hospital in Whitehaven), and the teams who support them – including domestics, estates staff, allied health professionals, receptionists, administrators and senior managers, walked the 84-mile length of the wall in three days. They raised an amazing £3,212!
May was also the month of collaboration as the Trust welcomed a senior psychiatrist and lecturer, Dr Kim Madundo to visit from Tanzania for four weeks, as part of an ongoing partnership. Organised by the Trust’s Medical Education team, the visit is part of a partnership between CNTW and the psychiatry department at the Kilimanjaro Christian Medical Centre (KCMC) in Moshi, Tanzania. The main aim of the collaboration is to share ideas, practices and research initiatives, so that both organisations can learn from each other.
The Trust’s Research and Development Team celebrated a win at the national Research and Development Forum. The team won sponsor choice runner up for their poster on audit processes. There were nearly 900 delegates and 105 shortlisted posters, so it was a tremendous achievement. The poster presented the audit process of how the team risk assess studies for audit selection, giving examples of how audits have improved research quality.
The Team at OpCourage also had cause for celebration as they were awarded the Provider Collaborative Specialist Services Award for its work with veterans at the Positive Practice in Mental Health Awards. The service, which was established in April 2023 provides specialist care and support for those due to leave the armed forces, reservists and those who have already left. It is developed by veterans, for veterans.
In June, Kristina Whitworth, who works as a Peer Supporter in Cumbria was shortlisted for the NHS/Keyworker of the Year, in Newsquest’s Pride of Cumbria Awards. Kristina’s own son has additional needs, and she has used her own experiences to find new ways to support other families and their children. Over the past few years this has included setting up a drop-in support group for the families of the children her team supports. She has also trained her dog, cockerpoo Honey, to be a qualified therapy animal.
Every year in June marks Volunteers week, and we celebrated as Paul Chappel reached an impressive 50 years at the Trust, having worked as a pharmacist, before becoming a volunteer. In 1974, Paul applied and was successful in the post of Chief Pharmacist at St George’s Hospital. Thirty years later he retired and trained for, and volunteered as, the first hospital chaplain in Northumberland. Paul became hospital chaplain in 2002. He is now fully retired but still volunteers three hours a week at the chapel at St George’s Park.
In July the Trust’s Public Health Team was shortlisted for a prestigious Nursing Times Award in the Public Health Nursing category. The nomination recognised the teams work in implementing national screening programme pathways for long stay patients in the Trust. Patients were supported to attend the five national screening programmes: bowel, breast, cervical, abdominal aortic aneurysm and diabetic eye screening, and the NHS England pilot pathway for targeted lung health checks.
August saw the Trust interviewing for its latest cohort of Registered Nurse Degree Apprenticeships. The Trust is the only NHS Trust in the region to offer the course, which allows aspiring nurses the opportunity to earn and learn. A staggering 498 people applied for the first intake. Of those who were shortlisted, 24 were offered a place. The apprenticeship, in conjunction with the University of Sunderland, offers applicants paid employment and education through a combination of learning and working in a nursing environment for over five years.
The SHINE fund, part of our charity, celebrated its 10th birthday in September. SHINE stands for Support, Hope, Inspire, Nurture and Empower, and aims to improve the experience of patients receiving care in our hospital and community services. The charity has made a decade of difference. Thanks to support from our community, staff, former service users, families and the public, SHINE has been able to bring hope, smiles and comfort to patients and their carers.
Our annual staff awards ceremony took place at the end of September which celebrates the achievements of our staff and volunteers. We received 1,483 entries into our awards this year and our judges had a very difficult task of selecting the finalists.
In October, Dr Jane Bourne, a Senior Drama Therapist was recognised for her contribution to her role and was awarded the inaugural Gold Award for excellence by NHS England’s Chief Allied Health Professionals Officer Professor Suzanne Rastrick OBE. The first of its kind, the award goes to individuals who have strengthened and supported the work of AHPs over the last ten years. It has been developed to acknowledge and celebrate excellence, where a significant contribution has been made by AHPs in England. Jane works on a children and young person’s inpatient ward. As the only Drama Therapist in the Trust, she uses creative ways for engagement.
More celebration in November when the Trust was announced by the National Trust as one of the recipients of the 49 ‘Trees of Hope’ Sycamore Gap saplings being gifted to individuals, groups and organisations across the UK. The 49 saplings represent the tree’s height at the time it was felled. The National Trust received nearly 500 applications for the saplings grown from the much-loved tree. In a fitting tribute, the sapling will be planted at Sycamore Unit at Northgate Park.
Christmas time saw the talented ‘MopHeads’ release a Christmas song named after St Nicholas Hospital, the hospital they work in. Peter Prest and Paul Hewitson, also known as the Mopheads work as cleaners for NTW Solutions. Their song, St Nicholas (A Joy for Christmas) was written to raise money for the SHINE fund. The song’s accompanying music video was filmed at the hospital’s Jubilee Theatre, which was turned into a winter wonderland for the occasion, complete with snow and decorations.
The New Year saw artwork from a patient in secure care services, featured in an exhibition at the Baltic Centre for Contemporary Art. The Almost Home exhibition is a partnership between Baltic and criminal justice arts Koestler Arts. The exhibition showcased a range of fine art, design, writing and music from people in prisons, secure hospitals and probation services in the North East.
In March and April, we saw wellbeing drop-ins take place as work on Hope Haven began. Hope Haven will be a 24/7 wellbeing hub in Whitehaven, and whilst building works take place, drop-in wellbeing workshops and the roving ‘wheels of wellness’ started to offer support. The Trust is working closely with several local organisations to provide support at Hope Haven, including iCan Wellbeing Group CIO, Whitehaven Community Trust, Cumbria Health, Everyturn Mental Health and Home Group.
Although 2024/25 has been a challenging year, our staff continue to do great work each day to provide the best possible care to those who need us.
Performance relating to the quality of NHS services provided
The CNTW Quality Account provides comprehensive information on performance in terms of the provision of quality services, including performance against mandated core indicators, quality indicators and the Trust’s quality priorities. Copies of the Quality Account can be obtained from the Trust’s website or the NHS website www.
Registration with the Care Quality Commission (CQC)
The Trust is required to register with the CQC, and its current registration status is registered without conditions and therefore licensed to provide services. The CQC has not taken enforcement action against the Trust during 2024/2025.
In 2018, the Care Quality Commission (CQC) conducted an inspection of our services and once again rated us as “Outstanding”. We are one of only eight Mental Health and Disability Trusts in the country to be rated as such, as of 1 April 2025.
During July and September 2024, the CQC conducted an assessment of all wards for people with a learning disability or autism. As of 31 March 2025, the Trust had not received the final assessment report. Further detail on the initial findings of the CQC assessment can be found in the Annual Governance Statement in section 2.10.
In February 2025, the CQC conduced a focused inspection of community mental health and early intervention in psychosis teams. As of 31 March 2025, the Trust had not received the draft inspection report.
NHS Oversight Framework 2024/25
NHS England’s NHS Oversight Framework provides the framework for overseeing providers and identifying potential support needs. The framework looks at five themes:
• Quality of care
• Finance and use of resources
• Operational performance
• Strategic change
• Leadership and improvement capability (well-led).
Based on information from these themes, providers are segmented from 1 to 4, where ‘4’ reflects providers receiving the most support, and ‘1’ reflects providers with maximum autonomy. A Foundation Trust will only be in segments 3 or 4 where it has been found to be in breach or suspected breach of its licence.
A new NHS Oversight Framework is being developed for release in July 2025 which will include published detailed data, a new set of measurements, and a fifth category.
Segmentation
NHS England have assessed the Trust as ‘segment 2’ – “Developing with confidence in the ability to improve further and operate in a high-functioning NHS system”. There are no enforcement actions placed upon the Trust by NHS England and no actions are being taken or proposed by the organisation. At Month 12 2024/25, the Trust reported financial surplus for the year end.
This segmentation information is the Trust’s position as of 31 March 2025. Current segmentation information for NHS Trusts and Foundation Trusts is published on the NHS England’s website.
Finance and Use of Resources
The Trust provides services to a broad range of commissioners. The main commissioners for the Trust in 2024/25 were as follows:
• North East and North Cumbria Integrated Care Board
• NHS England
• Cumbria and North East Commissioning Hub which is the local team of NHS England
• Integrated Care Boards out of area plus Scottish, Welsh, and Irish health bodies who commission on an individual named patient contract basis, and
• Local Authorities.
We continue to be the lead provider for specialised provider collaboratives for adult secure, children and young people’s services and adult eating disorder services, working in partnership with NHS England and Tees, Esk and Wear Valley NHS Foundation Trust. In October 2024, perinatal specialised services became a provider collaborative, adding to our lead provider contract. We are also lead provider for OpCourage (veteran’s) provider collaborative working in partnership with four NHS foundation trusts and two voluntary sector organisations to provide services for populations across the North East, Yorkshire and the North West.
Commissioners review our performance through monthly monitoring reports and regular contract meetings. The Trust provides routine commissioner data to the North East and North Cumbria Integrated Care Board (NENC ICB), allowing us to maintain our positive relationship with commissioners. Mental Health continues to be commissioned predominately on a block allocation basis. The foundation of the allocations are the totals identified through the pandemic based upon adjusted levels of expenditure from 2019/20. The totals have been adjusted for inflation, efficiency and development annually.
The Trust planned to deliver a £3.1m deficit as part of the North East and North Cumbria Integrated Care System. Ongoing discussions with commissioners resulted in changes to the Trust plan through the year. The Trust agreed in-year contract variations with NENC ICB and NHS England which revised the Trust plan to deliver a £2.4m surplus by the end of the financial year. Following revaluation of the leased assets held in the Trust’s subsidiary company, NTW solutions the 2024/25 accounts include a prior period adjustment to reflect an arising deferred tax asset. The adjusted financial performance for the CNTW Group for the period ending 31 March 2025 was £4.2m (2023/24 £58k). The adjusted financial performance is after exceptional items such as impairments and full details are reported within note 1.26 of the annual accounts.
The Secretary of State for Health and Social Care announced a major change to the organisational architecture of the NHS in March 2025. NHS England will be taken back into direct government control. The process is expected to take place over two years. While it is anticipated the changes will impact on the commissioning and regulatory arrangements in place details are yet to be announced.
The government announced its intention to develop a 10-year plan for the NHS. It is widely expected the NHS Trusts and Integrated Care Systems will be required to deliver longer term performance, workforce and financial planning through 2025/26.
Task force on climate related financial disclosures (TCFD)
NHS England’s NHS Foundation Trust Annual Reporting Manual has adopted a phased approach to incorporating the TCFD recommended disclosures as part of sustainability reporting requirements for NHS bodies, stemming from HM Treasury’s TCFD aligned disclosure guidance for public sector annual reports. TCFD recommended disclosures as interpreted and adapted for the public sector by the HM Treasury TCFD aligned disclosure application guidance, will be implemented in sustainability reporting requirements on a phased basis up to the 2025/26 financial year. Local NHS bodies are not required to disclose scope 1, 2 and 3 greenhouse gas emissions under TCFD requirements as these are computed nationally by NHS England.
The phased approach incorporates the disclosure requirements of the governance, risk management and metrics and targets pillars for 2024/25. These disclosures are provided in section 2.9 the Sustainability Report.
NTW Solutions Limited (Solutions) Performance
Financial Performance
The Trust’s subsidiary company is included within the financial performance for the group. All profits generated by Solutions are retained and reinvested by the Trust as part of the CNTW Group. The company did not issue any dividend payment in 2024/25. The annual accounts for Solutions will not be formally approved by the NTW Solutions Board until November 2025.
Service Level Agreements and Key Performance Indicators (KPIs)
NTW Solutions Limited have Service Level Agreements in place for all services. The Company monitors service performance at corporate level through agreed Key Performance Indicators (KPIs) at Leadership Team meetings, Company Board meetings and at joint monthly ‘Informed Client’ meetings and quarterly Strategic Liaison meetings with the Trust.
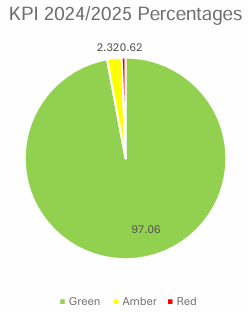
As of 31 March 2025, 141 KPIs were in place, (an increase from 134 the previous year). Of these, 116 hit their green expected target every month of 2024/25, 8 KPIs were not reported (on hold) by mutual agreement, leaving 17 KPIs where amber or red results were recorded. Any KPI recorded as “amber” or “red” i.e., not meeting agreed target levels, requires us to provide the Trust with an explanation or an action plan setting out how performance will be improved. Our KPIs are also reviewed twice per year by both the Company and the Trust to ensure they remain relevant, with appropriate target levels. 2025 saw an in-depth review of all service level agreements and their KPIs with all documentation agreed and re-signed by both NTW Solutions and the Trust.
Across the full year the Company reported on 1,609 KPI measurements, with 97.06% of these meeting the mutually agreed target, as shown in the chart below.
Other Benchmarking and Assessment Reports
For some services we are able to benchmark our performance with other NHS organisations or undertake self-assessment using national processes.
The ERIC Report (Estates Return Information Collection)
This is the main national annual benchmarking tool for NHS estates and facilities services. We compare performance against services in 45 Mental Health and Learning Disability Trusts. The majority of the many indicators for 2023/24 (the latest available data) placed us “mid-table” or better. This data set, as with other benchmarking tools, should be considered in the context of wider quality of service assessments, such as PLACE results, CQC inspections, cleaning audits, Degree Day Data (weather) etc.
The Premises Assurance Model (PAM) annual report
This report is based on self-assessment against 366 estates related questions covering safety, patient experience, efficiency, effectiveness and management of estates services. This data collection is now part of a national electronic submission (previously data was held locally by individual Trusts). National results are not yet being shared but the self-assessment submission showed a very positive position as in recent years. Any areas requiring improvement have action plans developed which are monitored in order to make improvements.
Patient Led Assessment of the Care Environment (PLACE)
Annual PLACE assessments are designed to provide motivation for improvement by receiving feedback directly from patients and others about how the environment or services might be enhanced. Our PLACE inspections have been undertaken, and our services compare well with others. A full report is due in 2025/26 and will be discussed at both Company Board and Leadership Team meetings. The report will also be reviewed by the Trust Quality and Performance Committee and Resource and Business Assurance Committee.
Mental health issues are common but one out of every six people who experience them say they face stigma and discrimination as a result. People with learning disabilities, autism and other disabilities and impairments also experience unfairness in many areas of life. CNTW aims to be a campaigning organisation which challenges discrimination of all types, and which has an important role to play in improving outcomes for people with mental health issues, learning disabilities and other disabilities in the region.
The Trust has in place an Equality, Diversity and Human Rights Policy which was updated in May 2022. The policy provides the overall framework for meeting the Trusts commitment to promoting equality, diversity, and human rights. The Trust recognises the need to tackle discrimination and to promote equality between different groups in the community, whilst also addressing the diverse needs of individuals and ensuring the upholding of human rights, ensuring fair treatment, protection of dignity and giving everyone the chance to play a full part in society. A review of the Policy is scheduled to take place in 2025/26.
Further information on our work to tackle discrimination and implementation of our policies and actions around ensuring equality, diversity and inclusion can be found in the Staffing report in section 2.3 and our Health Inequalities Annual Report 2024/25.
During the year, the Trust has engaged in discussions to ensure it takes a Trauma Informed approach in everything we do and was selected as a Quality Priority for 2024/25. Our Trauma Informed Care Lead has been leading work to define what we mean by trauma informed care. Trauma results from an event, series of events, or set of circumstances that is experienced by an individual as harmful or life threatening. While unique to the individual, generally the experience of trauma can cause lasting adverse effects, limiting the ability to function and achieve mental, physical, social, emotional, or spiritual well-being. Trauma-informed care does not mean assuming everyone has a history of trauma and adversity, but rather that the possibility is anticipated for each person we are in contact with. Everyone can benefit from services that are trauma-informed, but most mental health service users who have experienced trauma, will find it challenging to use services if they are not trauma informed. Another key element of the approach is to move from asking ‘what is wrong with you’ to ‘what happened to you’ and to really understand the impact of a person’s lived experience on them.
As part of our Quality Priorities for 2024/25 we looked at how we embed being trauma informed in everything we do, including our policies and pathways, our communication, leadership, and governance and how we make the organisation a trauma informed place to work. This was underpinned by seven key principles, collaboration/coproduction, empowerment, providing environments that are culturally, psychologically, physically, and sexually safe, offering choice, establishing trust, emphasising people’s strengths and minimising traumatisation/re-traumatisation.
A variety of tools were used to assess how well we are doing as a trauma informed organisation and to identify actions to support improvement in different areas of the Trust. A standard one-day training package was developed as part of the inpatient Quality Standard Framework with over 200 staff receiving the training in inpatient and secure services. This is also used to train staff in other settings in the Trust. Our training packages are co-produced with people with lived experience and a broader Trust wide training strategy and the development of a programmatic plan for trauma informed research has been commenced.
Several other large-scale initiatives have been completed during the year, including work on hate crime, sexual safety, development of an inpatient clothing bank.
A variety of sessions have taken place with focused groups, including a Culturally Inclusive Trauma-Informed Care session held to embed inclusion into practice, a session with the Disability Network to further ‘empower’ our staff with disabilities, Trauma informed Practice sessions for Chaplaincy and for our Workforce departments. The Trust Board of Directors and our Trust Leadership Forum have also engaged in sessions to think about how we become a truly Trauma Informed Organisation, and we have worked with workforce to develop key workforce policies to support our staff in a trauma informed way. More information on the impact of this work can be found in the Trust’s Quality Report.
Tackling Health inequalities
In 2024/25 the Board of Directors agreed five key priorities for tackling health inequalities in our services:
1. Developing the CNTW Patient and Carer Race Equality Framework (PCREF).
2. Implementing the Core20Plus5 for children and young people.
3. Developing CNTW’s role as an anchor institution – tackling the wider economic and social determinants of wellbeing.
4. Digital inclusion and accessibility.
5. Morbidity and mortality – addressing poor physical health outcomes among our patient populations (including implementation of the Core20Plus5 for adults).
Workforce Equality, Diversity and Inclusion (EDI) will also remain a priority for the Trust. This work is led by the Trust’s quality, Diversity and Inclusion Steering Group which will work closely with the Trust’s Health Equity Steering Group to ensure a joined-up approach to the Trust’s DI and health inequalities work.
Health Inequalities – Governance
We have agreed our health inequalities governance structure and established a Health Equity Steering Group which will oversee the delivery of our health inequalities priorities. The group is chaired by our Executive Director of Workforce and Organisational Development and includes representation from our three operational groups and relevant corporate teams. The Health Equity Steering Group reports into the Trust’s executive Management Group and will report to the Trust Board via the relevant Board Committees for each of the health inequalities workstreams listed above.
A new Patient and Carer Race Equality Framework Steering Group chaired by our Community Care Group Director (South) will provide oversight of the development and implementation of our PCREF plans and will report into the Health Equity Steering Group. We have incorporated our existing Health Equity Data and Evidence Working Group into the Trust’s formal governance structure. This group brings together analytical expertise from across the Trust and the North East Quality Observatory Service (NEQOS) and is chaired by our Director of Research and Clinical Effectiveness.
Delivery against our other priorities for tackling health inequalities will be integrated into existing Trust programmes and report into the Health Equity Steering Group monthly.
Health Equity Data and Evidence
Data and evidence are key to understanding inequalities and what works to address them. Successful delivery of the priority areas outlined above requires the analysis and monitoring of a significant amount of data and the translation of this data into actionable insights.
During 2024/25 our Health Equity Data and Evidence Group led the development of the Trust’s first Health Inequalities Annual Report with input from our patients and carers and is currently focused on the development of our PCREF dataset which will inform and help us to monitor our work to tackle ethnic and cultural inequalities in our services.
Our 2024/25 Health Inequalities Annual Report is published separately and is available on the Trust website alongside this report and includes data about inequalities in our services during 2024/25. The report focuses on inequalities linked to sex, age, ethnicity and deprivation in the following areas:
• Detentions under the Mental Health Act
• The use of restrictive interventions
• Children and young peoples’ access to Trust services
• Talking Therapies recovery
Patient and Carer Race Equality Framework
The Patient and Carer Race Equality Framework (PCREF) is an anti-racism, race equity and accountability framework for mental health Trusts and providers of publicly funded mental health services. NHS England requires all mental health Trusts to develop and publish their own Patient and Carer Race Equality Framework. This will be our Trust’s plan for tackling racism and inequalities linked to culture, faith and ethnicity in our services. To date our PCREF development work has focused on:
• Developing our PCREF dataset – collating ethnicity data across Trust services to understand inequalities.
• Bringing together leaders from minoritised communities to agree how we co-produce our PCREF plan in partnership with people from culturally and ethnically minoritised communities.
• Engaging patients and carers from racialised and culturally minoritised backgrounds who have experience using CNTW services and can contribute their perspective on how our services need to change in order to meet the holistic needs of people from all backgrounds.
We are also actively contributing to anti-racism work across the North East and North Cumbria system through our membership of the North East Anti Racism Coalition (NEARC) and Everyturn Mental Health’s PCREF Advisory Board.
Core20Plus5 for Children and Young People
Core20PLUS5 is the flagship framework of NHS ngland’s Healthcare Ine ualities Improvement programme. It aims to support coordinated activity to reduce health inequalities at national and system level by defining a target population cohort and five clinical areas of focus where work to address inequalities should be accelerated.
One of the five clinical areas of focus outlined in the Core20Plus5 for Children and Young People is improving access to mental health services for people aged 0-17 from different ethnicities, ages, sexes and areas of deprivation. During 2024/25 our Health Equity Data and Evidence Group has developed new analysis of inequalities in access to Trust services among children and young people, generating insights which will support our implementation of both the Core20Plus5 for children and young people and the development of our Patient and Carer Race Equality Framework.
Senior leaders from our Specialist Care Group are leading the development of our action plan for improving equity in access to our services for children and young people including the implementation of the Core20Plus5 framework, working collaboratively with partners across the system and integrating a health inequalities perspective into our children’s transformation work.
CNTW as an Anchor Institution
NHS Trusts have a duty to work closely with partners to improve population health both through service provision and through the development of their role as ‘anchor institutions’. Anchor institutions are organisations which operate in a specific place and will not move their operations elsewhere due to the nature of their work, and whose sustainability is linked to the wellbeing of their local populations. Through strategic management of their resources and operations, anchor institutions can help tackle the wider social, economic and environmental determinants of wellbeing.
CNTW is delivering a range of initiatives aligned to the broader anchor institutions agenda, including a significant amount of work aimed at widening access to employment with the Trust through a range of apprenticeships and work placement schemes and developing our contribution to system-level working to tackle health-related economic inactivity.
Digital Inclusion and Accessibility
Mitigating against digital exclusion is one of the five national priorities for tackling health inequalities previously identified by NHS England. In 2023, NHS England published a Digital Inclusion Framework which identifies five priority domains and actions for providers and NHS staff.
Published in 2023, CNTW’s Digital Strategy identifies key objectives for the Trust in relation to developing inclusive digitally-enabled care pathways. We are currently working to implement the national Reasonable Adjustments Digital Flag across CNTW which will enable us to deliver a more personalised experience of care which better meets the holistic needs of our patients, building on the successful introduction of a learning disabilities and autism digital flag in RiO (our patient record system). We are also supporting the development and implementation of the North East and North Cumbria Integrated Care System Digital Inclusion Plan, including the roll-out of a region-wide device repurposing scheme. Over the coming financial year, we will develop additional Trust-level projects aligned to national and regional digital inclusion priorities.
Morbidity and Mortality
CNTW provides care to patient groups that are likely to experience significantly poorer physical health outcomes than the general population. For many of our patients, poor physical health outcomes are not inevitable. During 2024/25 the Trust has developed in draft a Physical Health Strategy which outlines our approach to improving the physical health of people who use CNTW services over the coming years. We will adopt a targeted approach to this work which aims to tackle health inequalities within the CNTW patient population, working in collaboration with system partners to implement the Core20Plus5 for adults and ICS Guidance for improving the physical health of people with SMI.
Fraud prevention and management of interests
The Trust works closely with its Internal Audit Team including the Local Counter Fraud Service and support awareness raising of the potential for fraud. The Trust has a Declarations of Interest policy, reviewed, amended and approved by the Trust Audit Committee in 2025, aligned to NHS England requirements that all CNTW Staff must comply with to ensure the Trust is transparent in all business conduct. To support compliance with the policy, the Trust developed an online reporting system to enable all staff to easily declare any interests or potential interests they may have. The policy has been successful in providing clarity that it is the responsibility of all staff to declare interests to ensure they are impartial and honest in the conduct of their official duties. To ensure the Trust is transparent in all business conduct the declarations can be viewed on the Trust website or can be accessed on request by contacting Kirsty Allan, Deputy Trust Secretary, Chief Executive’s Office, St. Nicholas Hospital, Jubilee Road, Gosforth, Newcastle upon Tyne, NE3 3XT. (corporateaffairs
Important Post Year End Events
The directors have confirmed that there are no expected post balance sheet events which will materially affect the disclosures made within the Accounts 2024/2025. Overseas Operations The Trust does not engage in any commercial overseas operations.
James Duncan
Chief Executive
25 June 2025
2.1 Directors report 2024/2025
The Board of Directors
The Trust’s Board of Directors keeps its performance and effectiveness under continual review and undertakes an annual self-assessment of effectiveness. The Board also has a development programme and regularly reviews its governance arrangements. A regular review of the terms of reference and self-assessment exercise is also conducted on the Board and all committees.
During quarter 3 2024/25, the Trust commissioned an external review of the governance framework, and other key elements of the well led framework. ConsultOne were commissioned to undertake the review. The review was commissioned in the context of the changes within the Trust and its leadership during the previous 12-24 months, and changes to the governance framework to test the effectiveness of this in the context of being well led. The Trust sought an external perspective over three aspects of its governance arrangements:
• Board and committee governance, effectiveness, and ways of working (it was agreed that the Council of Governors would be excluded from this element as it was felt that this forum had recently been reviewed and subject to new ways of working and is operating effectively).
• Embeddedness of the Trust’s ‘With You in Mind’ strategy and plans to deliver this.
• Executive effectiveness with a focus on understanding and appropriateness of the executive director responsibilities and portfolios.
Each element of the review was subject to a separate report, recognising the different audiences and participation. The review included a broad range of activity including documentation review, one-to-one interviews, online survey, focus groups, meeting observations and research.
The outcome of the review was presented to the Board in February 2025 and overall, ConsultOne felt that the Board was in a good place with evidence of many areas of good practice. Feedback was positive including an improved position of Board diversity and a greater focus on Board development. They identified opportunities to strengthen the effectiveness and impact of the Board and for it to be more strategic and demonstrate greater ownership and ambition of its agenda. Refreshing and updating the Trust’s supporting strategies alongside greater specificity of outcome and measurement. Continuing improvements in the quality and focus of reporting including greater focus on assurance, escalation by exception and clarity of purpose and ask of reports.
The Board will review, oversee and monitor the outputs from the review during 2025/26.
The Board of Directors maintains continuous oversight of the Trust’s risk management and internal control systems with regular reviews covering all material controls, including financial, operational and compliance controls. The Board of Directors reports on internal control through the work of the Audit Committee and the Annual Governance Statement.
During the past 12 – 24 months, the Trust has been through a period of significant change. This includes changes in the Trust’s leadership of the organisation not only changes to the Executive Team structure and portfolios, but also the appointment of a new Chair of the Council of Governors and Board of Directors and newly appointed Non-Executive Directors. The Trust recognises the implementation of Integrated Care Systems and Integrated Care Boards and partnerships and the need to operate within a system that incorporates the NHS ICB structures. Alongside this, we have also made the following organisational changes:
• Implementation of a new strategy ‘With you in mind’ (from Spring 2023)
• A review of the Trust governance framework (during 2023/24)
• A review of the Trust risk management systems, processes, and policy (during 2023/24)
• A review of the Trust operational structures (implementation from April 2024)
On this basis, during 2023/24, a review of the Board Assurance Framework, Risk Management Policy and process was undertaken. Following the implementation of the Trust’s ‘With You in Mind’ strategy, all supporting strategies were withdrawn to enable a single strategy for the organisation to shape a clear direction, and culture. This included the withdrawal of the Risk Management Strategy for 2017-2022. Further information on the outcome of the review of risk management can be found in the Annual Governance Statement in section 2.10 and the Audit Committee report in section 2.10.
Alongside the review of the risk management policy and process, the Trust’s governance framework was also subject of review, led by the Director of Communications and Corporate Affairs during 2023/24 into 2024/25. An Internal Audit Advisory review on the new governance framework was undertaken in Q4 2023/24 with the final report published on 23 April 2024. Overall, the report noted a maturing but effective governance process operating at executive level with effective alignment between the Board's identified concerns and the focus of executive meetings. The report identified opportunities to formalise and better evidence the flow of assurances and escalation of matters of concern between forums which was one of the original drivers for restructuring executive level meetings and this has progressed significantly throughout the 2024/25 year.
NTW Solutions has its own Board of Directors. In accordance with the company’s Articles of Association, all proposed changes to the Articles of Association, and director appointments require the approval of the Trust Board and/or the Trust’s Chief Executive or his nominated representative, on behalf of the Trust’s Board of Directors as shareholder of the Company.
Chair and Non-Executive Director (NED) appointments
A term of office for the Trust Chair and NED is up to three years with a maximum of two terms of office. The Trust considers the need for progressive refreshing of the Board of Directors. Therefore, the Chair or a NED is subject to an annual appraisal of their performance, similar to the Chief Executive and Executive Directors. Any term beyond six years (i.e., two terms) is only made in exceptional circumstances and is subject to an annual re-appointment process which includes a rigorous review of performance and satisfactory appraisal. The Chair and all NEDs report the outcomes of their annual appraisal of their performance to the Council of Governors’ Nomination Committee.
The Council of Governors’ Nominations Committee is responsible for managing the process for the appointment and removal of a Trust Chair and NEDs. Circumstances that may lead to the removal of a Chair or NED include, but are not limited to, gross misconduct, a request from the Board for the removal of a particular NED, the Chair losing the confidence of the Board or Council of Governors and the severe failure of the Chair to fulfil the role.
The Trust Chair
During the period of 1 April 2024 – 31 March 2025, the role of Chair of the Board of Directors and Council of Governors was held by Darren Best who commenced his role with the Trust on 1 October 2023. The Chair is responsible for providing leadership to the Council of Governors and Board of Directors, ensuring good governance is maintained across the organisation. The Chair is also responsible for ensuring the integrity and effectiveness of the relationships between Governors and Directors. The Chair leads the performance appraisals of the Council of Governors, NEDs and the Chief Executive.
The Trust Vice Chair
During the period of 1 April 2024 to 31 March 2025, Brendan Hill held the role of Vice Chair. Brendan Hill was appointed into the role of Vice-Chair from 1 October 2023.
The Trust Senior Independent Non-Executive Director
David Arthur was appointed as the Senior Independent Director from 1 July 2021 until 14 January 2025 at which point, David has completed his second term of office. Michael Robinson was appointed into the role of Senior Independent Director from 15 January 2025 and continues to undertake this role. The Senior Independent Director leads the performance appraisal of the Chair.
The Chief Executive
The role of Chief Executive has been held by James Duncan since 1 February 2022. The Chief Executive’s principal responsibility is the effective running and operation of the Foundation Trust’s business. The Chief Executive is also responsible for proposing and developing the Trust’s strategy and business plan objectives in close consultation with the Chair of the Board of Directors. The Chief Executive is responsible for preparing forward planning information, which forms part of the Annual Plan, taking into consideration the views expressed by the Board of Directors and Council of Governors. The Chief Executive is responsible, with the executive team, for implementing the decisions of the Board of Directors and its committees and leads the performance appraisals of the Executive Directors and Director of Communications and Corporate Affairs/Company Secretary.
Directors’ skills, expertise and experience – CNTW Group
The Board of Directors believes that it continues to operate effectively. The Board keeps the size, composition, and succession of directors under review, in line with the Trust’s business objectives, and makes recommendations as appropriate to the Council of Governors and the Governors’ Nomination Committee via the Chair and Chief Executive. As a result of the work of the Nominations Committee and the Council of Governors relating to the Chair and NED appointment and reappointment process, the Trust formally acknowledged and accepted the recommendation that appointments to the Board should seek to ensure consideration of gender, equality, and diversity balance with the Board of Directors. The Trust continues to be committed to this recommendation and will ensure a strong focus on equality, diversity and inclusion is maintained as part of future appointment and re-appointment processes. The qualifications, skills, expertise and experience of the Trust’s directors as of 31 March 2025 are shown below.
Darren Best, Chair
• 30 years as a Police Officer with over a decade working in senior police leadership roles.
• Head of Professional Standards, Area Commander and Head of Criminal Investigation Department, Cleveland Police.
• Temporary Assistant Chief Constable, Durham Constabulary.
• Assistant Chief Constable and Deputy Chief Constable, Northumbria Police.
• Chair of Teesside Safeguarding Adults Board (October 2021 – April 2024).
• CNTW Non-Executive Director and Vice-Chair.
David Arthur, Non-Executive Director, and Senior Independent Director (until 14 January 2025)
• Chartered Accountant (1977).
• Fellow of the Institute of Chartered Accountants in England and Wales (1982).
• 40 years as a partner in Tait Walker LLP, Chartered Accountants.
• National head of Forensic Services of MHA, Chartered Accountants network.
• Chair of Percy Hedley Foundation.
• Trustee of Mental Health Concern, Chair of Finance Committee and Member of Governance Committee. • Chair of the Governors of Dame Allan’s Schools.
• Director and founder member of North East Fraud Forum.
• ICAEW representative on National Business Crime Forum.
• Member of North East Bank of England Panel.
• Chair of Bulman Property Limited.
• President of Northern Society of Chartered Accountants.
• Member of Business Engagement and Advisory Board Newcastle University.
Michael Robinson, Non-Executive Director and Senior Independent Director (Senior Independent Director from 15 January 2025)
• BA [Hons] in Law from Oxford University.
• Qualified Solicitor (now retired).
• Experienced non-executive director and board member.
• Former partner in the corporate department of a large UK-based law firm.
• Company Secretary and Group Legal Director at the Sage Group plc for 15 years.
Paula Breen, Non-Executive Director (until 31 March 2025)
• MA (Strategic Human Resource Management).
• Chartered Institute of Personnel and Development (CIPD) and Institute of Leadership and Management (ILAM).
• BA Business Management and Finance.
• Post Graduate Diploma in Education Leadership.
• Over 30 years business leadership in medium sized public and private organisations in both Executive and Non-Executive roles.
• Strategic Practice Management Primary Care, Northumberland.
• Managing Partner Primary Care, Cumbria.
• Chair and Head of Finance and HR Eden Primary Care Network, Cumbria.
• Chief Operating Officer Cumbria Education Trust.
• Elected Member and Cabinet Resources Portfolio Holder, Eden District Council.
• Founding Director (NED) Heart of Cumbria Ltd.
• Governor and Chair of Finance, Ullswater Community College.
• Director (NED) Eden Valley Hospice.
• Director of Finance and Resources and Company Secretary, Education.
• Group Chairman (NED) Coast and Country Housing Ltd.
• Director of Business Management, Norcare Ltd.
• Business Leadership Member, North East Region School Leaders Forum.
• Chair, North East Academies Forum.
• Board Member Darlington College.
Brendan Hill, Non-Executive Director and Vice-Chair
• Registered Mental Health Nurse. • Postgrad in Dip Mental Health Practice.
• 38 years working in health and care both in senior clinical and managerial positions.
• 17 years as CEO of national mental health charity Mental Health Concern and Insight IAPT.
• Executive Chair Bluestone Collaborative (VCSE development agency).
• Partner in Human Learning Systems Collaborative, supporting organisations to adapt and respond to complex systems.
• Trustee of Association of Mental health providers.
• Board member- Newcastle Well-being for Life Board.
• Chair of Chilli Studios (Community Arts Company).
• Chair of Mental Health Northeast (Regional infrastructure organisation).
• NED/Trustee for Charity – Ways to Wellness.
• Coaching and mentoring.
• RSA fellow.
Louise Nelson, Non-Executive Director
• PhD in Mental Health (Crisis resolution and home treatment- Service User experience).
• 37 years working in health with 20 years directly in mental health trusts and legacy institutions for Cumbria Partnership NHS Foundation Trust.
• 17 years working in Higher Education, culminating as Head of Nursing, Health, and Professional Practice at University of Cumbria.
• Previous role as Non-Executive Director for CPFT/NCUH and then NCIC.
• Chair of MIND Carlisle and Eden.
• Previous advisor for Borderline UK.
• Member of Quality Foundation.
• Volunteer for Project 5 offering mental health specialist support to NHS staff.
• Qualified and practising Executive Coach.
• Previous external advisor for Open University.
• Health and Wellbeing Champion for NCIC.
• Executive leadership in both Health and Education.
• Ofsted nominee for university first inspection in Health apprenticeship.
• Nursing education, clinical governance, and strategic planning.
Vikas Kumar – Non Executive Director
• 30+ years working in the creative and voluntary sector with over two decades working in senior leadership roles.
• Strategic Leadership - setting strategy, governance, programme development and delivery, innovation, financial management, fundraising, marketing, recruitment, coaching, mentoring, board development, quality assurance – specialising in EDI.
• Founder and Director of GemArts a visionary arts charity based in Gateshead.
• Extensive experience and knowledge working in partnership with cultural, public, private, and voluntary sector to engage with and deliver culturally relevant services to improve access and participation with Minority Ethnic communities.
• Awarded an MB in the 2017 Queen’s Birthday Honours list for services to Arts and Culture.
• In 2009 received the Gateshead Award by the Mayor for outstanding service to Gateshead.
• Awarded Asian Business Connexions Arts and Culture award in 2016, and then again in 2019.
• Appointed Deputy Lieutenant of Tyne and Wear in 2024
• Other Non-Exec roles include - Vice Chair and Trustee of Bensham Grove Community Centre; Trustee of Northern Stage; Member of Newcastle University Court and Nominations Committee.
Rachel Bourne – Non-Executive Director
• BA in History. • Member of CNTW Involvement Bank. • Woman and Non-Binary Officer for Student Union at Kings College, Cambridge. • Organised and chaired panel discussions on Learning Disabilities and discrimination in health and social care. • Involvement as a writer, speaker, and consultant for the national ‘Hearing the oice’ project an interdisciplinary study into voice-hearing. • Chaplaincy Assistant at Kings College Chapel. • Personal Assistant for Young People with Learning Disabilities and Epilepsy. • Assistant Regional Safeguarding Officer for the Methodist Church – North East. • Safeguarding Officer at Jesmond Methodist Church.
Robin Earl, Non-Executive Director
• Qualified Chartered Accountant.
• Group Executive Director at a house-building and regeneration company
• Executive Director of Corporate Services at a fast-growing charity providing services meeting complex health and social needs.
• Advisor to numerous local councils, the Welsh Government, and Scottish Executive on regeneration projects.
• Finance Director of an urban regeneration company in the North East of England.
• Project finance role with the National Regeneration Agency.
• Member of the Finance Committee at Newcastle Gateshead Initiative.
• Non-executive director of a housing association.
James Duncan, Chief Executive
• Degree in Politics and History.
• Chartered Institute of Public Finance and Accountancy).
• Extensive board experience in the NHS over 25 years.
• Significant experience in leading major and transformational programmes across Trusts and systems.
• Extensive work in public, service user and carer involvement.
• Experience in managing mergers, FT application process, PFI and significant capital investment.
• Has undertaken national leadership roles in financial and system development.
• Senior responsible officer for capital and estate development for the Integrated Care System.
Dr Rajesh Nadkarni, Deputy Chief Executive / Executive Medical Director
• FRCPsych, MMedSc in Psychiatry (University of Leeds).
• Doctorate of Medicine (MD).
• Diplomate of the National Board in Psychiatry from India and Bachelor of Medicine and Bachelor of Surgery (MBBS).
• 25 years’ experience as a forensic psychiatrist with extensive expertise in the clinical. assessment and management of people with mental health difficulties and involvement in criminal or court pathways.
• Continues to provide clinical expertise to the Newcastle Crown Court Mental Health Team and Northumbria Stalking Intervention Project.
• Provider Partner Board Member of the Integrated Care Board North East and North Cumbria.
• Member of GMC Advisory Forum on GMC procedures and doctors health.
• Member of the Mental Health Economics Collaborative, Mental Health Confederation.
• Member of the National Health and Justice Clinical Reference Group.
Ramona Duguid, Chief Operating Officer
• MBA, BA in Business Management.
• Over 25 years’ experience of working in the NHS.
• Strategic development and transformation delivery.
• Complex change management and stakeholder engagement.
• Operational delivery and performance management.
• Extensive experience in governance, risk management and regulatory compliance.
• Quality improvement and service development.
• Partnership working and integration.
Lynne Shaw, Executive Director of Workforce and Organisational Development
• MA in Human Resource Management.
• Post Graduate Certificate in Strategic Workforce Planning.
• BA (Hons) in Business Management. • Member of Chartered Institute of Personnel and Development (CIPD).
• 30+ years’ experience in the field of HR, including 20+ years in the NHS.
• Extensive experience of generalist HR, change management, transformational leadership, workforce development, training, organisational development, wellbeing, equality, diversity and inclusion, transactional HR processes.
• National NHS Aspirant HR Director’s Programme.
• Member of the National Healthcare People Management Association and Regional ice President for the North East and Cumbria.
• Co Chair of the regional HRD network.
Kevin Scollay, Executive Director of Finance
• Degree in Economics.
• Charted Institute of Management Accountants.
• Range of experience across NHS sectors o Acute (11 years) o Ambulance (3 years) o Commissioning (3 years)
• Previously Director of Finance at an NHS Foundation Trust.
• Experience in contracting, financial management and financial recovery.
Sarah Rushbrooke, Executive Director of Nursing, Therapies and Quality Assurance
• Registered General Nurse.
• Diploma in Professional Studies in Nursing.
• BSc (Hons) Nursing Science.
• Post Graduate Diploma with Commendation in Academic and Professional Learning.
• Msc Academic and Professional Learning.
• Nye Bevan Executive Leadership Programme.
• Extensive Nursing experience in NHS (39 years).
• Experience of implementing large scale change through quality improvement methodologies and qualifications.
• Extensive Experience in a wide range of nursing specialities and organisations including oncology, urology, elderly care, mental health and learning disabilities, surgery, urgent and emergency care.
• Director of Quality, Patient Safety, Innovation and Improvement at North East Ambulance Service.
• Director of Community Services and Deputy Chief Nurse at Royal Marsden NHS FT.
• Group Director South Locality at CNTW.
• Director of Quality and Patient safety at North of England Cancer Network.
• Deputy Director of Nursing, Quality & Safety at NHS England Cumbria, Northumberland, Tyne and Wear Area Team.
• Qualified Virginia Mason Production System Coach.
• Insights Discovery Facilitator.
Debbie Henderson, Director of Communications and Corporate Affairs/Company Secretary (non-voting)
• BSc (Hons), Sociology with Psychological Studies
• MSc Healthcare Management
Chartered Governance Institute (ACIS)
• 25 years’ experience in the NHS in the South West, North Yorkshire and North East across acute, community and mental health Foundation Trusts
• Substantial NHS experience in governance, service change, risk management, statutory/regulatory compliance, communications and engagement • Trustee, Vice-Chair and Senior Independent Director for RISE North East
Number of meetings and attendance
The Trust’s Board of Directors met formally 13 times during 2024/25 which included six extra ordinary Board meetings. The table below shows the members of the Board of Directors including their titles, attendance at Board meetings, the date of appointment and the expiry date of the current tenure of the Chair and each Non-Executive Director.
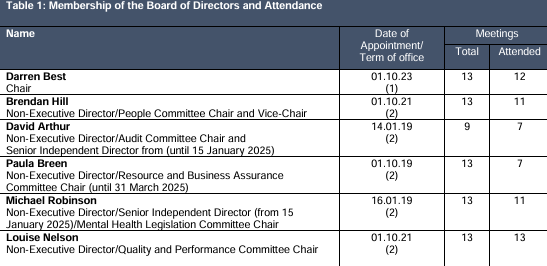
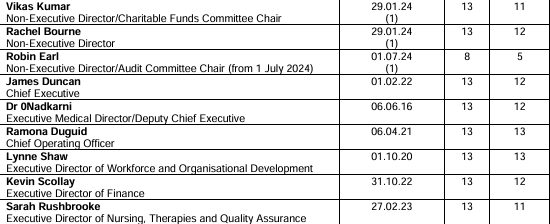
Independent Non-Executive Directors (NEDs)
The Board of Directors is satisfied that the NEDs, who served on the Board of Directors for the period under review were independent. The Board of Directors is satisfied that there were no relationships or circumstances likely to affect independence, and the criteria of the NHS Foundation Trust Code of Governance was considered in arriving at their view. This continues to be reinforced through the appointments/re-appointments process applied by the Governors’ Nominations Committee.
NTW Solutions Limited – Board of Directors
The qualifications, skills, expertise and experience of NTW Solutions Limited directors as of 31 March 2025 are shown below.
Malcolm Aiston, Non-Executive Director and Chair NTW Solutions
• Chartered Engineer with an Honours Degree in Engineering. • 40 years’ experience in NHS estates and facilities services. • Over 19 years as professional lead for these services in the Trust and its predecessor organisations. • Developing and leading implementation of strategic change, including overseeing major award-winning capital projects. • Experience in leading organisational change. • Membership of national estates forums. • Chair of Northern and Yorkshire NHS Apprenticeship Training Scheme for over 10 years. • Trustee of Pagabo Foundation a charity focusing on Mental Health in the construction industry.
Andrew Buckley, Non-Executive Director NTW Solutions (appointment commenced April 2019)
• BA in Modern Languages. • Masters in business administration. • Graduate Member of the Institute of Export. • 30 years commercial experience in marketing, sales, communications, business development and customer services. • Experience in leading organisational change. • Held senior level posts with Stanley Tools, Britvic, Seagram, The Sage Group, FTSE and Make UK. • Latterly Chief Executive with RTC North, a consultancy company helping businesses to innovate, compete and grow.
Tracey Sopp, Managing Director (Executive)
• Membership of the Chartered Institute of Public Finance Accountants (CIPFA). • 28 years’ experience in NHS financial services including e tensive experience in production of annual accounts, taxation, cash management, transactional processing and financial governance and systems. • Leading business transformation projects and delivering efficiency and process improvements. • Experience of leading a range of other business support services.
Matthew Lessells, Director of Estates (Executive)
• Chartered Engineer. • Master’s degree in building services engineering. • 30 years’ experience in the NHS estates in both acute and mental health services. • Experience in leading organisational change. • Membership of national estates forums. • Volunteer as Blood biker supporting Northumbria blood bikes.
Kevin Scollay, Shareholder Representative for the Trust
• Degree in Economics. • Charted Institute of Management Accountants. • Range of experience across NHS sectors o Acute (11 years) o Ambulance (3 years) o Commissioning (3 years) • Previously Director of Finance at another NHS Foundation Trust. • Experience in contracting, financial management and financial recovery.
The NTW Solutions Board of Directors met 11 times in the year. Table 2 below shows the members of the Board during 2024/25, date of appointment and attendance at Board meetings.
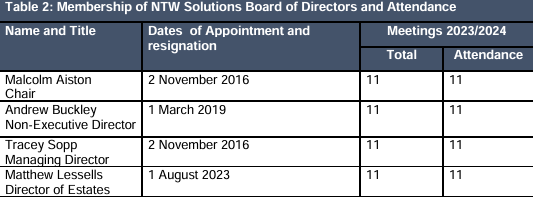
The Trust’s Constitution requires the Board to convene a Remuneration Committee and an Audit Committee and any other committees as it sees fit to discharge its duties. As a mental health provider, the Trust is also statutorily required to convene a Mental Health Legislation Committee.
The Board of Directors annually reviews and approve changes to the terms of reference for the Board and its committees. The Trust undertook a review of the terms of reference of the Board and Board committees in June 2024. A further review of the Board and Committee terms of reference is scheduled to take place at the April 2025 Board meeting.
As part of its last comprehensive inspection by the CQC, the Trust governance was reviewed through the Well Led domain, gaining an ‘Outstanding’ outcome in this area, as well as being rated as ‘Outstanding’ overall in both 2016 and 2018 following the CQC Well Led review and comprehensive review of services.
In addition to the Remuneration Committee, Audit Committee and Mental Health Legislation Committee, there are three other standing Board committees delivering an assurance function. These are, the Resource and Business Assurance Committee (RABAC), the Quality and Performance Committee (Q&P), and the People Committee.
Each committee is chaired by a Non-Executive Director, supported by other Non-Executive Directors, as well as Executive Director Leads and subject experts to ensure receipt of appropriate assurance. The delegated responsibilities of each committee in relation to risk management is reviewed by the Audit Committee underpinned by regular reviews of the Trusts Board Assurance Framework (BAF), which provides information on key risks to achieving the Trusts strategic ambitions. Each BAF risk is aligned to the relevant Board Committee for ongoing review and assurance. Each committee annually self-assesses its effectiveness annually against its terms of reference. The Audit Committee has implemented an annual cycle of reporting for Board Committee Chairs to attend meetings of the Audit Committee and provide an update on their processes for assurance in relation to the management of risks within their remit.
A full review of the Trust’s Standing Financial Instructions (which NTW Solutions SFIs incorporate) and Scheme of Reservation and Delegation was undertaken and approved by the Trust Board in February 2025. The Scheme of Reservation and Delegation of NTW Solutions reserves the company’s audit and director remuneration functions to be overseen by the Trust’s Audit Committee and Remuneration Committee. This includes the reporting of the company’s risk management arrangements to the Trust’s Audit Committee. A full review of the NTW Solutions Scheme of Delegation was undertaken and approved by the Trust Board in September 2023, and it is scheduled for a further review in October 2025.
NTW Solutions Limited Board committees and governance structure
NTW Solutions’ Board has established two Board committees:
• The Health, Safety and Security (HSS) Committee – meets quarterly, and which is chaired by the Managing Director. Matters of concern are escalated for board discussion and/or decision, as per the Terms of Reference. The HSS Committee self assesses its effectiveness annually and the NTWS Board of Directors reviews and approves any changes to its terms of reference.
• The Risk, Assurance and Governance (RAG) Committee – established in May 2024 and which meets monthly, chaired by the Managing Director. The RAG Committee provides assurance to the board on matters of governance and risk. Matters of concern are escalated to the Board for discussion and/or decision as per the Terms of Reference.
Both of the Committees self-assesses their effectiveness annually and the NTW Solutions Board reviews and approves any changes to the Terms of Reference of the Committees.
The NTW Solutions Leadership Team includes its senior leaders who meets monthly with a focus on operational matters that enable the company to achieve its strategic objectives.
The Trust’s Executive Director of Finance attends the NTWS Board as the Shareholder Representative.
Fit and Proper Persons Test
All Directors on the Board of Directors have, on appointment, confirmed that they met the Fit and Proper Persons Test and completed an annual declaration that they continue to be a fit and proper person in accordance with the Health and Social Care 2008 (Regulated Activities) Regulations 2014 Regulation 5: Fit and Proper Persons Requirement.
The Trust’s Fit and Proper Persons Policy was reviewed and updated in-year in line with the new NHS England Fit and Proper Persons Framework that came into effect from 1st October 2023.
Register of Directors’ Interests
The Trust maintains a formal Register of Directors’ Interests. The Register is available for inspection on the internet at www.
NTW Solutions Ltd maintains a formal Register of Directors’ Interests. The Register is available on request to Sarah Jones, Director of Legal and Commercial Services/Company Secretary, Arran House, St Nicholas Hospital, Jubilee Road, Gosforth, Newcastle Upon Tyne, NE3 3XT.
HM Treasury, cost allocation and charging guidance
The Group and Trust has complied with cost allocation and charging guidance issues by HM Treasury. Political Donations The Group and Trust did not make any political donations during 2024/25. No Directors have personal membership/donation payments in place to political parties and these are declared and available on the Trust website.
We continue to monitor our performance in terms of paying our trade suppliers in line with our target of paying 95% within 30 days of receiving a valid invoice or within term, whichever is the shorter. An analysis of our performance is shown in the table below.
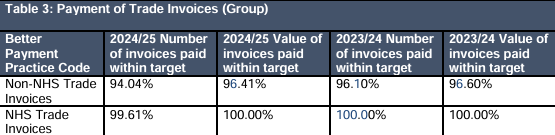
The Group and Trust had no interest on late payment of commercial debts or compensation paid to cover debt recovery costs as at 31 March 2025 (31 March 2024: £nil).
NHS England’s well-led framework
The Trust’s Annual Governance Statement 2024/25 (section 2.10) outlines how the Trust has regard to NHS England’s well-led framework, in arriving at its overall evaluation of the organisation’s performance, internal control and Board Assurance Framework.
The CQC undertook a well led review and inspection of core services in April 2018 and found the Trust to be ‘Outstanding’ overall, and in the Well Led, Responsive, Caring and Effective domains and ‘Good’ in the Safe domain. The Trust commissioned an external review of its governance arrangements against the Well Led Framework, using the Good Governance Institute in 2021/22. The Trust undertook a further independent review governance and elements of the well led framework in quarter 3 of 2024/25. Further detail is available the Annual Governance Statement in section 2.10.
The Trust has applied the principles of the NHS Foundation Trust Code of Governance on a comply or explain basis. The NHS Foundation Trust Code of Governance April 2023 is based on the principles of the UK Corporate Governance Code. The Trust confirms that there are no material inconsistencies between:
• The Annual Governance Statement.
• The Annual Report.
• Reports arising from Care Quality Commission planned and responsive reviews of the NHS Foundation Trust and any consequent action plans developed by the NHS Foundation Trust.
The Trust remains fully compliant with the requirements of the NHS Code of Governance as outlined in section 2.7 and reported to the Audit Committee in May 2025.
Lived Experience Service
The Patient and Carer Involvement Service has changed its name to the Lived experience Service to acknowledge the increasing responsibilities of the Service and the growing Lived experience workforce across the Trust.
The Lived experience Service provides two service domains which now better reflect their purpose. The Patient and Carer Involvement Service will now be known as the Involvement Service and the Peer Support Service will now be known as the Lived Experience Support Service.

The Lived Experience Service coordinates and facilitates service user and carer involvement on behalf of operational services and the Trust, underpinning and supporting the ethos of the Trust’s strategies ‘With You in Mind’ and ‘Together: Service user and carer involvement strategy’.
Involvement Service
The Involvement Bank is a way for service users and carers, who are not paid employees of the Trust, to have their say and help shape services. Service users and carers (also known as Contributors) who join the Involvement Bank can choose to be involved in areas of interest to them. An offer of a recognition payment is available in acknowledgement of their contributions.
Membership of the Involvement Bank continued to grow during 2024/25, increasing from 255 active Contributors at the end of March 2024, to 349 Contributors at the end of March 2025.
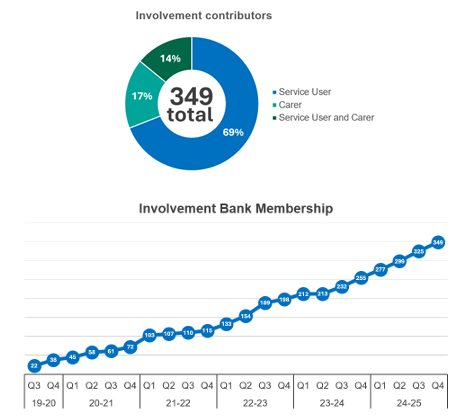
Involvement activities demonstrate how operational services, and senior managers involve Contributors (service users and carers) in making decisions. Involvement activity requests have continued to increase at a significant rate, with 82% of requests received in the year 2024/25 having been fulfilled.
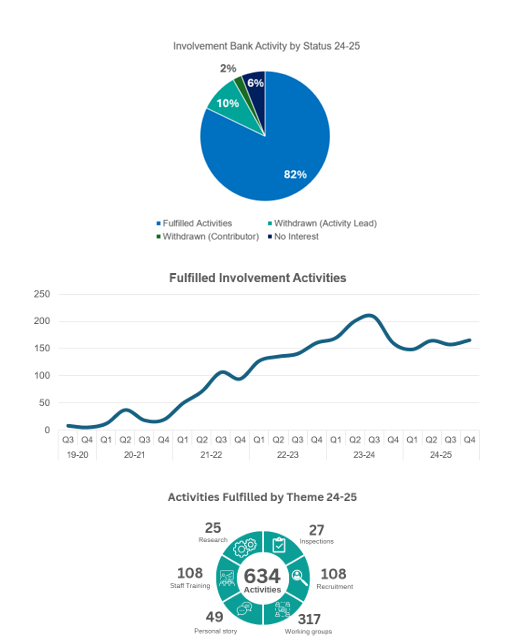
Youth Involvement Bank (YIB)
The Youth Involvement Bank now invites eligible 11- to 17-year-olds (13-17 years for inpatients) who have lived experience of services offered by the Trust (within the last 4 years) to get involved. 10 Contributors were registered on the YIB at the end of March 2025, and they fulfilled 9 activities during 2024/25.

Public Involvement
The service supports involvement activity outside of the Involvement Bank process, this is known as Public Involvement. With an alternative offer of support for co-creation, co-design and co-production opportunities which can benefit from the Involvement Service acting as an Activity Lead on behalf of operational services and senior management, for programmes or external involvement projects.

Provider Collaboratives
Provider Collaboratives are partnerships that bring together two or more NHS Trusts to work together at scale to benefit their populations.
North East and North Cumbria (NENC) Mental Health, Learning Disability and Autism Partnership, made up of Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust (CNTW) and Tees, Esk, and Wear Valleys NHS Foundation Trust (TEWV), have commissioned four Provider Collaborative services, which each have a Lived Experience Advisory Group (LEAG). These are:
• Children and Young People Mental Health Inpatient Services
• Adult Low and Medium Secure Services
• Adult Eating Disorder Services
• Perinatal Mental Health Services The Lived Experience Service support processing payments and attending the L AG’s to 52 support meaningful involvement.
Recognition Payments
Recognition payments have increased in line with the growth of the involvement activities being supported:
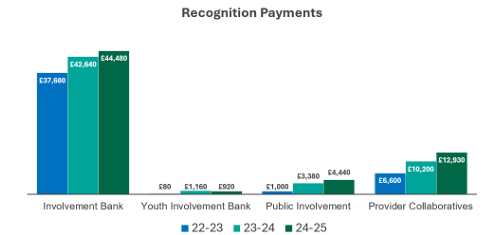
Triangle of Care
As one of the quality priorities for the Trust in 2024/25, the six key principles of the Triangle of Care (ToC) are designed to ensure families, friends and carers are better involved and informed in the provision of care and supported in their caring role, creating an inclusive culture where carers, service users and staff work together to ensure excellent health care is provided across all service areas.
A Trust wide assurance process includes an annual review of performance, in respect of all operational services, against the principles. The Triangle of Care Annual Report 2024 demonstrated evidenced practice and was submitted to the Carers Trust for evaluation and assessment. The Trust was successful in retaining its two-star accredited status.
Carers Together Advisory Group
The Carers Together Advisory Group undertake focussed evaluations providing considered recommendations for improvements to service design, systems, processes, and resource. Some of the work undertaken in 2024 has been the review and relaunch of the ‘Together: Service user and Carer involvement strategy’, the co-production of the ‘Carer Record Practice Guidance Note’ and the review of the ‘Getting to Know You as a Carer’ guidance.
Lived Experience Support Service
The Lived Experience Support Service works in partnership with clinical operational services to deliver a development and wellbeing model that enables the peer support workforce to thrive and grow in line with all other professions within the Trust. Peer Supporters are employed directly by and work into clinical services, or employed through the voluntary sector, and are supported through this development and wellbeing framework.
Clinical services across the organisation continue to provide specialist peer support to our service users and carers with 98 Peer Supporters in post at the end of March 2025.
The career pathway for Peer Supporters allows them to stay within their specialism with Senior Peer Supporter and Peer Support Supervisor positions embedded into clinical services.
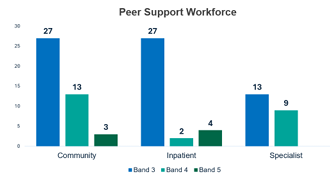
Lived experience positions outside of mental health support roles are developing in the Trust, further work is being undertaken to improve the offer of non-operational lived experience roles. The Family Ambassador role within the Children and Young Peoples Service Provider Collaborative, offers support to the families of the children and young people in inpatient services.
A newly appointed ADHD programme manager is working on design and delivering an ADHD programme in Cumbria for 12 months, with the first cohort starting in June. Referrals for service users are now open in the North Cumbria locality.
User and Carer Reference Group
The Service User and Carer Reference Group (also known as the Reference Group) is a bi-monthly lived experience engagement platform which provides service users and carers, partnership and third sector organisations in the North East and North Cumbria an opportunity to use lived experience to influence change, jointly with Trust staff. The group is directed by a steering group and chaired by service users and carers.
•Margaret Adams, Co-Chair
•George Moat, Co-Chair
•Heather Lee, Co-Chair
•Fatema Rahman, Co-Chair
The Group meets six times a year, at an external accessible venue in Newcastle upon Tyne and has been delivered bi-monthly throughout 2024/25.

Recovery College Collaborative
The Trust works in partnership with Recovery Colleges across its geographical footprint. They deliver comprehensive, peer-led education and training programmes and are run like any other college, providing education as a route to recovery, not as a form of therapy with courses co-devised and co-delivered by people with lived experience of mental illness.
Service user Feedback
Service user feedback is actively sought and reviewed through several initiatives which are supported through the Trust’s dedicated Service User and Carer Engagement Team and quality assurance functions including:
Your Voice – Survey
In April 2024 we moved to our new co-developed service user and carer experience survey Your Voice. Some highlights from the first year of Your Voice are:
•6,239 surveys were completed by service users and carers, 4,247 of these were completed by a service user and a further 576 were completed for a service user when they could not do this unaided. 1,206 surveys were completed by a carer. 210 surveys were completed where no option was chosen.
•185 teams and wards received feedback in the year.
•The Friends and Family Test (FFT) score for the year was 8.6 out of 10, this score is around average when compared with mental health providers nationally. National average in January 2024 was 8.9.
•From April 2024 there have been 15,546 themed comments, of which, 74.1% were positive.
•The main themes discussed by service users and carers were Communications, Patient Care and Values and Behaviours.
•624 You Said – We Did posters have been routinely produced.
In the last year, 6,239 surveys were completed by service users and carers. 4,247 of these were completed by a service user, 576 were completed by someone supporting a service user to share their experience, 1,206 were completed by a carer, relative or friend of a service user and 210 were completed by someone who shared an experience of a service without letting us know if they were a service user or a carer.
With the introduction of Your Voice, we took the opportunity to review how we could reach more service users and carers in a cost effective and environmentally friendly way opposed to just by mail. We now send a link for completion online via email and text and sending by mail is the last option we now use. Between April 2024 – March 2025 we have sent:
•13,344 emails
•33,083 texts
•10,642 letters
All question in the Your Voice experience survey offer the opportunity for service users and carers to share their experiences through a text box function. These comments are themed by the Commissioning and Quality Assurance team and included in a dashboard that all staff can access.
The comments as well as being themed into positive, negative and neutral are also assigned a main and sub-theme.
The most common theme for compliments has remained ‘ Values and Behaviours’ across all years, with staff being ‘Kind/Caring/Friendly’ being the most discussed sub-theme of this main theme.
You Said – We Did
You Said – We Did (YSWD) is a monthly opportunity for teams to respond to the themes that emerged in the previous month. This happens through choosing a comment from a service user or carer that is representative of a dominant theme and responding as a team.
YSWD has been used informally by many wards and teams in the Trust for many years. A centralised system is available to all wards and teams to support being responsive to experience feedback as a monthly process.
The system is attached to the Your Voice dashboard and was designed to be a simple 2 step process that any staff member can carry out, without the need for ratio access.
YSWD is ‘Listen’ and ‘Do’ part of the NHS England » Ask Listen Do – feedback, concerns and complaints process that Your voice supports. Something that the CQC are actively looking for evidence of during their visits. See the infographic below that e plains the process and how Your voice and YSWD fit into this process.
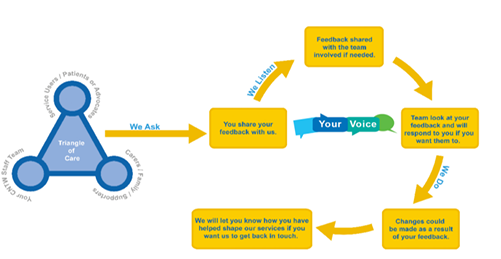
Quality priorities
Significant work has been undertaken to review our progress against the Quality Priorities set last year, and to agree our priorities for 2025/26. further detail can be found in the Trust’s Quality Account which can be obtained from the Trust’s website www.
Each year we set annual Quality Priorities to help us to achieve our long term Quality Goals. The Trust identifies priorities in partnership with service users, carers, staff and partners from their feedback, as well as considering information gained from incidents and complaints, and by learning from Care Quality Commission findings.
CNTW will maintain commitment to progressing work across the previous 4 Safety Themes and look forward to incorporating one new goal in relation to improved Medicines Safety.
•Reduce levels of Restrictive Practice
•Reduce levels of violence and aggression towards staff and patients
•Reduce levels of self harm
•Improve the management of physical health care.
•Improve medicines safety.
To achieve these goals, 12 priority areas have been identified:
•Risk assessment and management (including safety planning)
•Collaborative and person centred care planning
•Enhancing communication with families and carers
•Accurate, relevant and efficient clinical record keeping.
•Assertive engagement of those with Serious Mental Illness (SMI)
•Waiting list management
•Transitions
•Management of the deteriorating patient
•Sexual safety
•Inpatient areas – 10 high impact actions
•Sedative medication and risk of cardiorespiratory arrest
•Severe clozapine induced constipation
Work in these areas will be reported on during 2025/26, to provide a strong governance, assurance and oversight of delivery.
Service improvements following staff or service user surveys or CQC reports.
During 2024/25 there has been a significant amount of work undertaken to continue to deliver the quality priorities identified for the year.
Quality Priority 1 Implementation of PSIRF (Patient Safety Incident Response Framework)
•Continued alignment with the four PSIRF aims.
•Panels (PSLIP) were operational with Group representation added to strengthen learning integration.
•System based learning approaches like Early Learning Reviews ( LRs) and After Action Reviews (AARs) remain active and under continuous review.
•PSIRF maturity audit planned with "Audit One" and development of a Patient Safety Partners plan in Q4.
Quality Priority 2: Safety 5 Improvement Themes
•Themes include violence Reduction, Physical/Public Healthcare, Self Harm/Suicide Reduction, and Reducing Restrictive Practice.
•Violence Reduction has made strides in response to new NHS England guidance and targeted ward level strategies.
•Physical Health group re established; audits conducted and new strategies in development with an emphasis on improving health equity and outcomes in smoking cessation, obesity and metabolic syndromes.
•Reduction of Restrictive Practices work has led to significant reduction in use of Prone, Mechanical Restrain Equipment (MR ) and Seclusion in most services.
•Agreement to roll our ‘Sleep Well’ initiative across Inpatient, Specialist and Secure settings.
Quality Priority 3: Triangle of Care (ToC)
•Annual review of performance and co production of Triangle of Care Annual Report 2024 completed successfully.
•The Trust retained its Star 1 and 2 accreditations from the Carers Trust.
•Ongoing refinement of Carer Awareness Training and documentation.
Quality Priority: 4 Research and learning
•Learning and Improvement webinar established as a regular monthly session, supported by a cross CNTW steering group.
•Staff Research Community created to engage staff and build service connections.
•Research conference held on 2nd April 2025, with greater representation of all disciplines, people with lived experience and carers.
•Bespoke research learning webinars launched, covering topics such as data use, evaluation techniques, critical appraisal, and learning organisation principles.
Quality Priority 5: Embed Culture of Trauma Informed Care (TIC)
•A variety of tools were used to assess how well we are doing as a trauma informed organisation and to identify actions to support improvement in different areas of the Trust.
•A standard one day training package was developed as part of the inpatient Quality Standard Framework; over 200 staff have been trained in inpatient and secure services; this is also used to train staff in other settings in the Trust.
•A broader Trust wide training strategy and the development of a programmatic plan for trauma informed research has been commenced.
•All training and benchmarking were co produced with people with lived experience.
•Several other large scale initiatives have been completed, including work on hate crime, sexual safety, development of an inpatient clothing bank.
•A variety of sessions have taken place with focused groups, including a Culturally Inclusive Trauma Informed Care session held to embed inclusion into practice, a session with the Disability Network to further ‘empower’ our staff with disabilities, Trauma informed Practice sessions for Chaplaincy and for our Workforce departments. The Trust Board of Directors and our Trust Leadership Forum have also engaged in sessions to think about how we become a Trauma Informed Organisation.
•We have worked with workforce to develop key workforce policies to support our staff in a trauma informed way.
More detailed information on our progress against our Quality Priorities for 2024/25 can be found in the Trusts Quality Account on our website at www.
Patient Information
The Trust’s Patient Information Centre aims to ensure that everyone has access to a range of useful health and wellbeing information resources. The service is free and completely confidential. The staff at the Centre can provide access to information resources about: medical conditions, procedures and treatments and using the NHS complaints process and NHS services within the Trust.
The services offered by the Centre are available to everyone. The Centre has established good working relationships with other statutory and voluntary organisations so that they can make referrals with confidence. 800+ service user and carer information leaflets, including 23 mental health self-help guides are available online in a range of formats, including British Sign Language (BSL), Easy Read, Large print and audio www.
Our newly rebuilt website is AAA accessible within the context of the Web Content Accessibility Guidelines (WCAG), representing the highest level of accessibility compliance.
Complaints and Compliments
The Trust acknowledges that it is important for patients and their families and carers to know how to raise a concern or complaint and that a robust system is in place to investigate complaints thoroughly to raise confidence in our services and improve the patient experience. Comments, compliments and complaints are valuable learning tools and provide information that enables services to improve. The Trust’s Complaints Policy and accompanying Practice Guidance Notes provide the framework in which they can be managed effectively in line with the Local Authority, Social Services and National Health Service Complaints (England) Regulations 2009 (2009 Complaints Regulations) and the Parliamentary Health Service Ombudsman’s ‘Principles of Good Complaint Handling’ and the values of the Complaint Standards Framework.
We are confident that service users, carers and families know how to raise an issue or a complaint. Complaints can be made in writing, by telephone or by email. Information gathered through our complaints process is used to inform service improvements and ensure we provide the best possible care to our service users, their families and carers.
Complaints have increased during 2024/25 with a total of 816 received during the year. This is an overall increase of 37 complaints (5%) in comparison to 2023/24 and the highest number of complaints received per annum to date.
The Community Care Group accounted for 72% of the complaints received, followed by the Inpatient Care Group with 15% and the Specialist Care Group with 11%. The other 2% of complaints related to the non-clinical directorates.
Of note regarding the three highest complaint categories: patient care, communication and values and behaviours:
•Complaints related to patient care increased by 10%
•Complaints relating to communications increased by 4%
•Complaints relating to values and behaviours decreased by 15%
Complaint categories which have significantly increased in comparison to 2023/24 are:
•Complaints relating to admissions and discharges have increased by 26%
•Complaints relating to appointments have increased by 28%
•Complaints relating to prescribing have increased by 42%
Complaint categories which have significantly decreased in comparison to 2023/24 are in relation to waiting times which have decreased by 19%.
In 2024/25 we responded to complaints in line with agreed timescales in 94% of cases which is a 12% increase in comparison to 2023/24 and reflects the ongoing improvements made since the team staffing levels have been at full capacity.
The Patient Advice and Liaison Service (PALS) gives service users and carers an alternative to making a formal complaint. The service provides advice and support to service users, their families, carers and staff, providing information, signposting to appropriate agencies, listening to concerns. We can also signpost complainants to local advocacy services who offer support and advice around making a complaint.
In addition, we now have access to the Interpreting Service and can request interpreters for complainants who are deaf or do not use English as a first language.
If a complainant is dissatisfied with the outcome of a formal complaint investigation, they are given the option to contact the Trust again to explore issues further. However, if they choose not to do so then Stage 1 of the NHS complaints procedure has concluded. If they remain dissatisfied, they have the option to refer their complaint to the Parliamentary and Health Service Ombudsman (PHSO). This is known as Stage 2 of the NHS complaints procedure.
The role of the PHSO is to consider further independent investigation of complaints where individuals feel they have been treated unfairly or have received poor service from government departments and other public organisations and the NHS in England.
The Trust-wide Safety Group receives weekly reports on complaints received and triaged for investigation and extensions requests to keep Trust Directors informed and ensure they have oversight of the process. The Quality and Performance Committee reviews the complaints received and identifies trends which are outlined in the monthly and quarterly Quality and Safety reports. A bi-annual review of themes from complaint action plans is also circulated Trust-wide with the aim of improving the quality of care.
Stakeholder Relations
The Trust is a partner in the North East and North Cumbria Integrated Care System (ICS). The Trust is a member of the NENC Integrated Care Board (ICB) Mental Health, Learning Disabilities and Autism Executive Committee (MHLDA). We have continued to work in each locality to support the implementation of the five-year forward view including through Health and Wellbeing Boards, Integrated Care Partnerships and Place-based arrangements including health care providers, local authorities and third sector organisations.
We have a positive relationship with the main health scrutiny committees in each locality. Directors and senior clinical managers attend the Health Overview and Scrutiny Committee (OSC) meetings to present updates on the Trust’s plans, quality priorities and delivers specific presentations on any proposed changes to services.
For service changes, the Trust continues to work closely with relevant Commissioners to undertake any formal consultation processes or engagement associated with service developments including ensuring appropriate engagement and involvement.
Income disclosures as required by section 43(2A) of the NHS Act 2006 (as amended by the Health and Social Care Act 2012).
The statutory limitation on private patient income in section 44 of the 2006 Act was repealed with effect from 1 October 2012 by the Health and Social Care Act 2012. The Health and Social Care Act 2012 requires Foundation Trusts to make sure that the income they receive from providing goods and services for the NHS (their principal purpose) is greater than their income from other sources. This income has had no impact on the on the provision of goods and services for the purposes of the health service in England. The Private Patient Income for 2024/25 is shown in the table below.
| Table 4: Private Patient Income | ||||
|---|---|---|---|---|
| Private Patient Income |
Group 2024/25 £ |
Trust 2024/25 £ | Group 2023/24 £ | Trust 2023/24 £ |
| Private patient income | 0 | 0 | 0 | 0 |
| Total patient related income | 646,828 | 593,825 | 562,613 | 562,036 |
| Proportion (as percentage) | 0 | 0 | 0 | 0 |
The statutory limitation on private patient income in section 44 of the 2006 Act was repealed with effect from 1 October 2012 by the Health and Social Care Act 2012. The Health and Social Care Act 2012 requires Foundation Trusts to make sure that the income they receive from providing goods and services for the NHS (their principal purpose) is greater than their income from other sources.
James Duncan
Chief Executive
25 June 2025
Annual statement on remuneration
Members of the Board of Directors are the individuals who have responsibility for controlling the major activities of the Group including the Trusts’ subsidiary companies, and their remuneration is included in this report. This is in line with the requirement to include those who influence the decisions of the Group as a whole rather than decisions of individual directorates or business units within the organisation.
The Trust has a Remuneration Committee, whose role is to determine and review all aspects of the remuneration and terms and conditions of the Chief Executive and other Executive Directors and to agree associated processes and arrangements including appointments and Terms of Conditions. The Remuneration Committee is chaired by the Trust Chair and its membership is comprised of all Non-Executive Directors (NEDs). The Chair of the Board of Directors makes this annual statement as Chair of the Remuneration Committee, whose remit covers Executive Directors, and as Chair of the Council of Governors (Nominations Committee), whose remit covers NEDs.
In October 2024, the Remuneration Committee met to review the annual pay increase for Very Senior Managers (VSMs). Each year, as part of the public sector pay round, the government remits each pay review body to make recommendations for health service staff. NHS VSMs fall within the remit of the Senior Salaries Review Body (SSRB). The Secretary of State for Health and Social Care accepted the SSRB’s pay recommendations in full on 29 July 2024 in a Written Ministerial Statement announcing the pay award for VSMs as an across-the-board increase of 5%, backdated to 1 April 2024.
As in previous years, medical directors employed on the consultant contract should receive the agreed pay award for their consultant pay, as recommended by the Doctors and Dentists Review Body (DDRB). The management allowance payment received as part of their total remuneration package would receive the 5% increase.
NHS England’s Guidance on pay for SMs sets out thresholds where Trusts should seek ministerial approval/comment where a Chief Executive’s or Executive’s pay exceeds the agreed levels. However, this is not required where the sole reason for pay going above the relevant threshold is due to implementing the SSRB’s pay recommendations therefore there is no further action was required. Additional funding for VSM pay awards was provided as part of the pay award allocation adjustments as allocations do not separate out VSM pay from the wider pay bill. On this basis, the Committee approved the 5% pay increase for CNTW Executive Directors and NTW Solutions Directors noting the Medical Director increase was applicable for the management element only.
Darren Best
Chair
25 June 2025
Senior Managers’ Remuneration Policy
The Trust complies with all aspects of the NHS Code of Governance. This includes the main principle that:
‘Levels of remuneration should be sufficient to attract, retain and motivate directors of quality, and with skills and experience required to lead the NHS Foundation Trust successfully, but an NHS Foundation Trust should avoid paying more than is necessary for this purpose and should consider all relevant and current directions relating to contractual benefits such as pay and redundancy entitlements’.
The term ‘very senior manager’ includes all individuals who have held office as a member of the Trust Board of Directors and Directors of NTW Solutions Limited. Very senior managers remuneration comprises basic pay and NHS pension contribution only (variations are salary sacrifice benefits as set out in the table). This applies to all very senior managers. No performance related pay applies to very senior managers.
There are no provisions for the recovery of sums paid to senior managers or for withholding the payments of sums to senior managers.
During 2024/25, the Trust has had three substantive Executive Directors paid more than £150,000, the Chief Executive Officer, the Executive Medical Director and the Chief Operating Officer. The Trust is satisfied that the pay packages are reasonable.
The executive Medical Director’s package includes a sum for clinical duties as set out in table 7 remuneration reflects the complexity of the role and its responsibility.
All substantive Executive Directors' contracts are permanent with three months' notice (except the Chief executive whose notice period is 6 months) and all executive Directors’ termination payments (including redundancy and early retirement) were as per the general NHS terms and conditions applicable to other staff.
Performance related pay did not apply during 2024/25 and benefits in kind relate to lease cars and salary sacrifice schemes.
No non-contractual payments were made during 2024/25.
The Trust pays a fee to Non-Executive Directors which is detailed in table 7.
The Trust reimburses the Chief Executive, Executive Directors, and Non-Executive Directors any reasonable travelling, hotel, hospitality and other expenses wholly, exclusively and necessarily incurred in the proper performance of their duties. This is subject to the production of relevant invoices or other appropriate proof of expenditure in respect of claims submitted.
Policy on payment for loss of office
In accordance with the Senior Managers’ Remuneration Policy, all Executive Directors’ termination payments (including redundancy and early retirement) are aligned to the general NHS terms and conditions applicable to other staff.
Statement of consideration of employment conditions elsewhere in the Foundation Trust
Pay for other directors, senior managers and all other non-medical and dental staff is in accordance with the national Agenda for Change terms and conditions, (except for a small number of senior staff who have been appointed onto a single point within a local pay range, using the flexibilities within Agenda for Change for bands 8C and above). Pay for medical staff is in accordance with the national terms and conditions of service for hospital, medical and dental staff, and may include clinical excellence awards.
Policy on diversity and inclusion used by the remuneration committee.
When appointing senior managers to the Trust, the Remuneration Committee aligns with the Trust’s strategy to deliver Workforce Race Equality standards, Workforce Disability Equality Standards and increase inclusive leadership, as a Stonewall diversity champion. The Trust values and promotes diversity and is committed to equality of opportunity for all. The Trust believes that the best Boards are those that reflect the communities they serve, and applications are particularly welcomed from women, people from the local black and minority ethnic communities, and disabled people who we know are under-represented in senior manager roles.
Table 5: Future policy table
| Component of Pay | Link to Strategic Objectives | How the Trust Operates this in practice | Maximum Limit | Performance Measures |
|---|---|---|---|---|
| Basic Salary | To enable the Trust to attract and retain the highest calibre of senior leaders in a competitive market place through offering appropriate but attractive salary packages. | Executive Directors salaries are monitored using national benchmarking. Non-Executive Director salaries are also benchmarked to provide assurance that salaries remain appropriate. |
No prescribed maximum limit, however, salaries over £150,000 are subject to external opinion. | Annual appraisal of performance against agreed personal and corporate objectives. |
| Taxable Benefits | N/A | N/A | N/A | N/A |
| Pension | N/A | Via the NHS Pension Scheme | Standard NHS Pension Scheme | N/A |
| Bonus | N/A | N/A | N/A | N/A |
| Earn-back | N/A | N/A | N/A | N/A |
Annual report on Remuneration
Service Contracts obligations
The date of service contracts, unexpired term, and details of the notice period of Executive Directors who have served during the year are disclosed below and within the Accountability Report.
Remuneration Committee and Disclosures required by Health and Social Care Act
The purpose of the Remuneration Committee is to decide and review the terms and conditions of office of the Chief Executive and Executive Directors in the CNTW Group, comply with the requirements of the NHS Code of Governance and any other statutory requirements. The Remuneration Committee’s terms of reference are included on the Trust website, and its role includes agreeing processes and arrangements (and receiving and considering the outcome and recommendations from such processes) for approval, e.g., interview processes. Ensuring compliance with the requirements of “NHS Employers: Guidance for employers within the NHS on the process for making severance payments” was added to the committee’s remit during 2013/14 following instruction from, at the time, NHS Improvement.
All Group executive Director’s appointments and terms of office are considered by the Remuneration Committee. This includes the Chief Executive, whose appointment must be agreed by the Council of Governors.
The Council of Governors is responsible for the appointment/reappointment of the Chair of the Board of Directors and Council of Governors and NEDs with the associated work carried out by its Nominations Committee, which provides the Council of Governors with recommendations. The work of the Nominations Committee is described later in this report.
The Remuneration Committee is chaired by the Trust Chair and its membership is made up of all NEDs. The Remuneration Committee met twice during 2024/25. The table below shows the membership of the Remuneration Committee during 2024/25.
Table 6: Membership of the Remuneration Committee and Attendance during 2024/25
| Name | Meetings Total | Meetings Attended |
|---|---|---|
| Darren Best | 2 | 2 |
| David Arthur (until 15 January 2025) | 2 | 2 |
| Paula Breen | 2 | 1 |
| Michael Robinson | 2 | 1 |
| Louise Nelson | 2 | 0 |
| Brendan Hill | 2 | 2 |
| Rachel Bourne | 2 | 2 |
| Vikas Kumar | 2 | 1 |
| Robin Earl | 2 | 1 |
The Remuneration Committee has received advice from James Duncan, Chief Executive, Lynne Shaw, Executive Director of Workforce and Organisational Development and Debbie Henderson, Director of Communications and Corporate Affairs/Company Secretary to assist their considerations. Members of the Trust in attendance at meetings in an advisory capacity only are not in attendance during discussions of their own remuneration and/or Terms and Conditions.
The Council of Governors has established a Nominations Committee to provide it with recommendations relating to the appointment of the Chair and Non-Executive Directors and the associated remuneration and allowances and other terms and conditions. Details of the work of the Nominations Committee is included in the section on “Disclosures set out in the NHS Foundation Trust Code of Governance”.
During 2024/25, there were 14 individuals fulfilling the role as Director in the Trust, six of them receiving expenses in the reporting period totalling £6,380.49. The equivalent for 2023/24 for the Trust was 14 individuals, with four receiving expenses totalling £3,363.64.
During 2024/25, there were four individuals fulfilling the role as director in the Trust subsidiary company NTW Solutions, two of them receiving expenses in the period totalling £395.76. The equivalent for 2023/24 for the Trust subsidiary company NTW Solutions was five individuals, with three receiving expenses totalling £189.64.
During 2024/25, there were 38 individuals in Governor roles. Four Governors received expenses during the year which totalled £445.28The equivalent for 2023/24 was 37 individuals in Governor roles. Seven Governors during 2023/24 received expenses totalling £445.28.
CNTW Board of Directors remuneration – Salaries and pension entitlements for Board members who served during 2024/25 along with prior year comparatives.
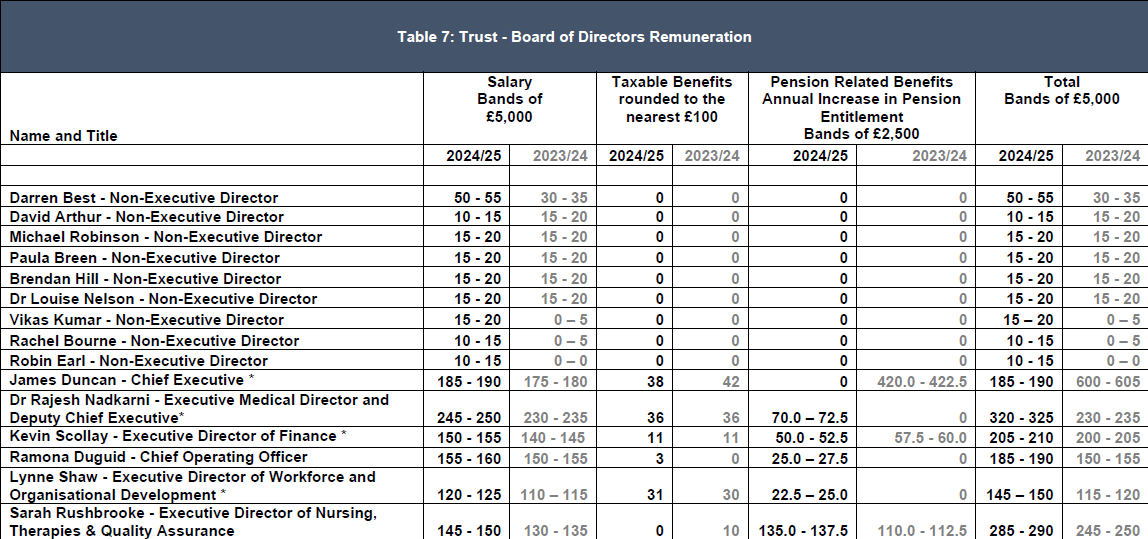
For Dr Rajesh Nadkarni, £32,000 of the remuneration relates to clinical duties (2023/24 £25,000). The remuneration of all other Executive Directors relates to management posts.
*The Directors highlighted with * have salary sacrifice schemes during the year, which can result in increases/decreases in both salary and pension related benefits as salary sacrifice schemes are entered into and withdrawn from. All taxable benefit costs are met by the employee as part of the salary sacrifice scheme arrangements.
NTW Solutions Board of Directors Remuneration - Remuneration for NTW Solutions Board members who served during 2024/25 along with prior year comparatives.
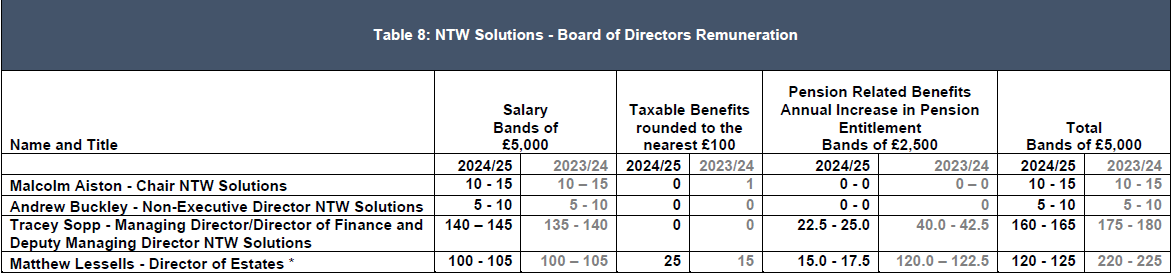
The Directors highlighted with * have salary sacrifice schemes during the year which can result in increases/decreases in both salary and pension related benefits as salary sacrifice schemes are entered into and withdrawn from.
Fair Pay
Reporting bodies are required to disclose the relationship between the remuneration of the highest paid director / member in their organisation and the 25th percentile, median and 75th percentile of remuneration of the organisation’s workforce. Total remuneration of the employee at the 25th percentile, median and 75th percentile is further broken down to disclose the salary component.
The banded remuneration of the highest paid director in the organisation in the financial year 2024/25 was £247,500 (2023/24 £232,500). This is a change between years of 6.5%. The relationship to the remuneration of the organisation's workforce is disclosed in the below table.The total remuneration includes salary, benefits in kind, but not severance payments. It does not include employer pension contributions and the cash equivalent transfer value of pension.
For employees of the Trust as a whole, the range of remuneration in 2024/25 was from £6,750 to £249,371 (2023/24 £6,750 to £231,076). The percentage change in average employee remuneration (based on the total for all employees on an annualised basis divided by the full- time equivalent number of employees) between years is 5.4%. No employees received remuneration in excess of the highest paid director / member in 2024/25 (There were none in 2023/24).
The remuneration of the employee at the 25th percentile, median and 75th percentile is set out below. The pay ratio shows the relations between the total pay and benefits of the highest paid director (excluding pension benefits) and each point in the remuneration range for the organisation’s workforce
| 2024/25 | 25th Percentile | Median | 75th Percentile |
|---|---|---|---|
| Salary component of pay | 26,925 | 34,411 | 46,148 |
| Total pay and benefits excluding pension benefits* | 26,925 | 34,411 | 46,148 |
| Pay and benefits excluding pension: Pay ration for the highest paid director | 9.19 | 7.19 | 5.36 |
*CNTW do not pay performance bonus to managers
| 2023/24 | 25th Percentile | Median | 75th Percentile |
|---|---|---|---|
| Salary component of pay | 25,266 | 33,021 | 43,742 |
| Total pay and benefits excluding pension benefits* | 25,266 | 33,021 | 43,742 |
| Pay and benefits excluding pension: Pay ration for the highest paid director | 9.20 | 7.04 | 5.32 |
*CNTW do not pay performance bonus to managers
The overall percentage difference has reduced as the highest paid direct / member remuneration includes elements not subject to the NHS annual pay uplift whereas this is applied in full to the remuneration of the employee at the 25th percentile, median and 75th percentile.
Total pension entitlement
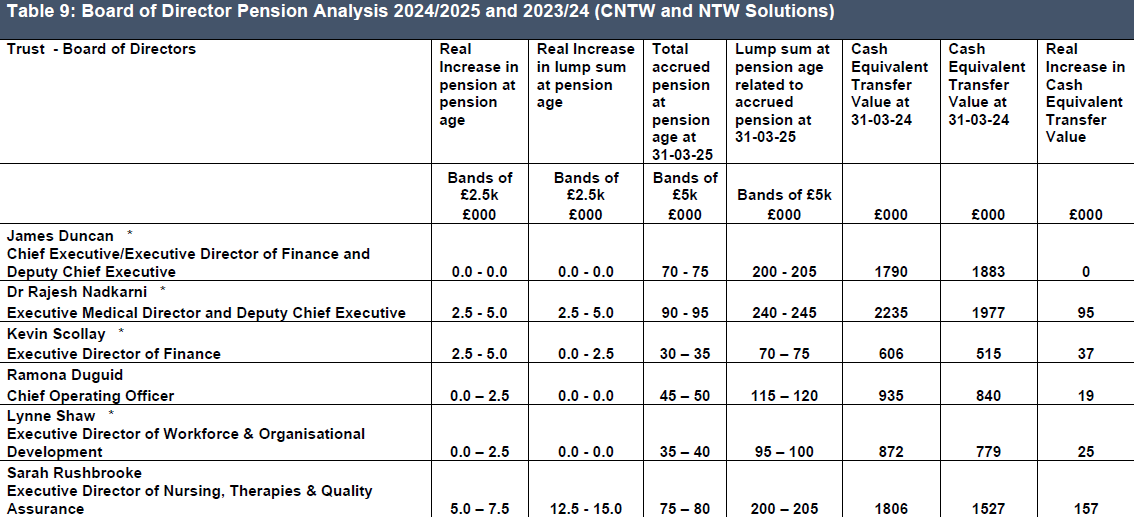
The Directors highlighted with * have salary sacrifice schemes during the year which can result in increases and decreases in pension benefits as schemes are entered into and withdrawn from.
Negative values are not disclosed in this table but are substituted with a zero.
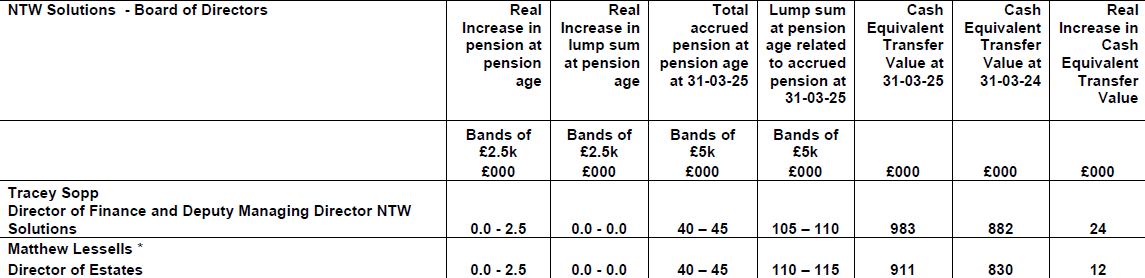
The Directors highlighted with * have salary sacrifice schemes during the year which can result in increases and decreases in pension benefits as schemes are entered into and withdrawn from.
Negative values are not disclosed in this table but are substituted with a zero.
The remuneration and pension benefits tables disclosed have been subject to audit and an unqualified opinion has been given.
Cash equivalent transfer values are not applicable where individuals are over 60 years old.
As Non-Executive members do not receive pensionable remuneration, there will be no entries in respect of pensions for Non-Executive members.
The Cash Equivalent Transfer Value (CETV) is the actuarially assessed capital value of the pension scheme benefits accrued by a member at a particular point in time. The benefits valued are the member's accumulated benefits and any contingent spouse's pension payable from the scheme. CETVs are calculated within the guidelines and framework prescribed by the Institute and Faculty of Actuaries.
The method used to calculate CETVs has changed to remove the adjustment for Guaranteed Minimum Pension (GMP) on 8th August 2019. If the individual concerned was entitled to GMP, this will affect the calculation of the real increase in CETV. This is more likely to affect the 1995 Section and the 2008 Section. This does not affect the calculation of the real increase in pension benefits, or the total pension related benefit figures disclosed.
Real Increase in CETV - This reflects the increase in CETV effectively funded by the employer. It takes account of the increase in accrued pension due to inflation, contributions paid by the employee (including the value of any benefits transferred from another pension scheme or arrangement).
The pension benefits and related CETVs disclosed do not allow for any potential future adjustments which may arise from the McCloud judgement.
Payments for loss of office
During 2024/25, no payments have been made to senior managers for loss of office.
Payments to past senior managers
No payments have been made to past senior managers during 2024/25.
![]()
James Duncan
Chief Executive
25 June 2025
Employee Numbers
As of 31 March
2025, the Board of Directors for Cumbria, Northumberland, Tyne and Wear Foundation Trust comprised of six Executive Directors (three female and three male) and eight Non-Executive Directors (three female and five male).
The Directors for NTW Solutions comprised of two Directors (one female and one male) and
two Non-Executive Directors (two male).
For the purposes of this Annual Report only Board members are considered to be
very senior managers.
The CNTW Group has 8929 employees including Non
-Executive Directors (6739 female and 2190 male) of whom 28% work part-time.
2523 employees (1877 female and 646 male) are also registered with one or more of the
Trust’s staff banks. In addition, there are currently 482 ‘bank only’ workers (309 female and 173 male) who do not hold substantive posts elsewhere in the Trust. A total of 451 current bank only staff worked shifts during 2024/2025.
Information on staff turnover can be found at NHS workforce statistics - NHS England Digital
Health and Wellbeing of our Staff
The Trust is committed to improving the health and wellbeing of its people and is continuously reviewing and updating our offer based on feedback from the engagement work we carry out across the organisation.
The health and wellbeing offer available to our staff is centred around the strategic health and wellbeing approach, depicted as a Star which represents an inclusive, diverse, and holistic health and wellbeing offer and incorporates the vision within the NHS People Plan and People Promise. This model provides a comprehensive framework to prioritise wellbeing across the organisation and ensures that health and wellbeing initiatives are transparent, allowing staff to easily identify the support available to them.
The Trust has successfully delivered a comprehensive programme of health and wellbeing offers in 2024, shifting towards a more proactive approach and culture. A total of 26 health and wellbeing campaigns were launched and showed an increase in participation and engagement.
In addition, the Workforce Development Team launched a monthly Health and Wellbeing newsletter achieving over 6,000 views and positive feedback, providing staff with a dedicated resource featuring the latest events and information. This sits alongside our ‘Thrive’ website which continues to be a dedicated resource for our staff.
From 1 April 2024, our Occupational Health provider moved to Optima Health following a tendering exercise. Management of the service is via monthly contract review meetings and the monitoring of Key Performance Indicators.
Each year, the Trust participates in the Better Health at Work Award which allows us to work closely with other sectors across the region to share learning and good practice. In January 2025, the Trust received confirmation of being awarded ‘Maintaining Excellence’ for the eighth consecutive year. This achievement highlights our ongoing commitment to supporting staff wellbeing and reflects the input of our teams who support this area across the organisation, all of whom play a role in helping support the wellbeing of our staff.
The Board and its Committees receive regular updates from the Trust’s Health and Wellbeing Steering Group on the current work taking place and further plans in relation to health and wellbeing across the Trust to embed the actions and principles of the NHS People Promise. This gives organisational assurance and evaluation against the wellbeing approach and wider Trust, regional and national initiatives.
To support the delivery of the Trust’s offer, the Trust’s Health and Wellbeing Lead attends both regional and national networks as a community of practice to source expertise, collaborate and support more efficient and effective practices, which feed into the Trust’s health and wellbeing ambitions.
Looking ahead to the next steps for 2025, we will continue the final stages of reporting to establish a health and wellbeing benchmark of the organisation against the NHS Employer’s Diagnostic Tool, which is designed to support NHS Organisations to create a culture of wellbeing that is right for its people. The diagnostic tool will enable the organisation to shape its health and wellbeing priorities and feed into the Trust priorities as well as informing the future agenda of health and wellbeing activity. Completing the tool will help identify three to five strong, evidence-based recommendations or themes which will shape the organisation’s future health and wellbeing ambitions as part of being a great place to work, as outlined in the Trust’s “With You in Mind” Strategy.
Another priority for the coming year is to embed the Sexual Safety Charter for our staff in response to changes in legislation.
Sickness Absence
Absence management continues to be a priority with the continuation of support for the workforce with underlying health conditions, neurodiversity, and complex lifestyles.
Both long term and short-term absence is monitored to ensure staff receive the right support, referring to the regional wellbeing hub where necessary. Reasonable adjustments, support via access to work and flexible working options are in place with a view to keeping staff at work.
| Figures Converted by DH to Best Estimates of Required Data Items | Statistics Produced by NHS Digital from ESR Data Warehouse | |||
|---|---|---|---|---|
| Average FTE 2024-25 | Adjusted FTE days lost to Cabinet Office definitions | Average Sick Days per FTE | FTE-Days Available | FTE-Days Lost to Sickness Absence |
| 8,040 | 116,142 | 14.4 | 2,934,478 | 188,409 |
Workforce Policies
The Trust is committed to maintaining a suite of workforce policies that are current, legally compliant, and reflective of both national guidance and evolving best practice. Policies are reviewed and updated on a regular basis, aligned with changes to employment legislation, amendments to national NHS terms and conditions of service, and emerging trends in people management. Each policy review includes a thorough equality impact assessment and a training needs analysis to ensure accessibility, fairness, and practical implementation across the organisation.
This work is enhanced by engagement with a wide range of stakeholders across the Trust, including staff networks, subject matter experts, and trade union representatives, ensuring our workforce policies are inclusive, responsive, and shaped by those they impact most.
As part of our ongoing strategic commitment to becoming a more trauma-informed organisation, we have also begun taking active steps to reflect this approach across our policies and practices. This includes renaming and reframing key policies to better align with compassionate and person-centred principles. For example, our Absence Policy has been updated and is now the Health, Wellbeing and Attendance Policy, and our former Grievance Policy has been redesigned as the Resolution Policy. These developments are directly aligned with our Trust strategy, 'With You in Mind', ensuring that the emotional and psychological wellbeing of our workforce is a core consideration in everything we do. Training on these policies will be rolled out for all managers across the Trust during 2025.
Equality, Diversity & Inclusion Objectives 2024/25
During 2024/25 we began work on the Equality Diversity and Inclusion Objectives that were agreed at Trust Board at the end of 2023. The objectives set are:
• Eliminate conditions and environment in which bullying, harassment and physical harassment occurs.
• Addressing progression within the Trust for staff protected under the Equality Act 2010.
•Engaging with racialised and ethnic minority communities to identify and agree core organisational competencies requiring further development.
Progress is being made against NHS England’s Equality Diversity and Inclusion Improvement Plan. Key areas we will need to continue to work towards are:
• Create and implement a talent management plan to improve the diversity of executive and senior leadership teams and evidence progress of implementation, the roll out of our new Leadership Programme will contribute to this.
• Work in partnership with community organisations, facilitated by Integrated Care Boards working with NHS organisations and arms-length bodies, such as the NHS Race and Health Observatory.
• Have mechanisms to ensure staff who raise concerns are protected by their organisation. We know from the bullying survey that we conducted this year that we still need to work towards ensuring that all our staff feel safe and supported to raise a concern. There will be an opportunity to refresh our approach to this with new Freedom to Speak up Guardians and consider how Freedom to Speak up Champions could play a bigger role.
Patient and Carer Race Equality Framework (PCREF)
Work has commenced on developing our PCREF. A meeting took place at the end of September with Community Leaders that established next steps for the work. We have collated data in line with the Framework’s technical guidance that will continue to inform our discussions with communities to co-produce a set of actions early in 2025/26.
Workforce Race Equality Standard (WRES)
The most recent WRES and Workforce Disability Equality Standard (WDES) Annual Report (2024/25) was published in August 2024. The data compiled within this report is from a snapshot taken on 31 March 2024, as well as findings from the most recent NHS Staff Survey which took place in Autumn 2023.
| Metric |
CNTW Figures for Latest Reporting Period White |
BME | Comments |
CNTW Figures for Previous Reporting Period White |
BME | Comments | 2024 Trend (2023 in Brackets) |
|---|---|---|---|---|---|---|---|
| Non-clinical Staff | 1495 | 47 | BME 11% of total workforce | 1548 | 52 | BME 9.06% of total workforce | BME workforce has grown |
| Clinical Staff | 5536 | 685 | BME 11% of total workforce | 5387 | 509 | BME 9.06% of total workforce | BME workforce has grown |
| Medical Staff | 166 | 165 | BME 11% of total workforce | 152 | 153 | BME 9.06% of total workforce | BME workforce has grown |
| Non-Clinical Band 5 or below | 1160 | 39 | 3% of non-Clinical staff are BME | 1243 | 43 | 3.2% of non-Clinical staff are BME | 82.9% BME (82.5%) vs 77.6% (77%) white staff in Band 5 or below Marginal change based on previous |
| Clinical Band 5 or below | 2572 | 543 | 10.9% of Clinical staff are BME | 2566 | 374 | 8.6% of Clinical staff are BME | 79.3% BME (73.5%) vs 46.5% white staff (47.6%) in Band 5 or below. Significant growth during reporting period. Planning and monitoring for progression will be key. |
| Medical Consultant Grade | 121 | 91 | 49.2% of Medical staff are BME | 116 | 88 | 50.2% of Medical staff are BME | 55.1% BME (43.1%) vs 72.8% white (56.8%) Consultant Grade staff |
| Staff appointed from shortlisting | 759 (3517 short listed) | 276 (1918 short listed) | White applicants 1.48 times more likely to be appointed | 1405 (4128 short listed) | 215 (1339 short listed) | White applicants 2.12 times more likely to be appointed | Improvement over the last 4 reporting periods |
| Staff entering formal disciplinary process | 54 | 12 | BME staff 1.76 time more likely to be in formal process | 76 | 12 | BME staff 1.57 times more likely to be in formal process | Slight deterioration |
| Staff accessing non-mandatory training & CPD | Not recorded by Group Workforce Teams and therefore unable to be reported on. | - | - | Due to staff not accessing non mandatory training during the pandemic, was not possible to calculate the figure. The 2020 return showed that BME staff were 1.5 times more likely than White staff to access non mandatory training. | - | - | - |
| % Staff experiencing bullying, harassment or abuse from patients, relatives or public | 24.7% | 36.55% | 11.85% point disparity gap | 26.6% | 36.2% | 9.6% point disparity gap | Experience of white staff has improved between 2022 to 2023, with marginal deterioration for BME staff. The disparity gap has increased |
| % Staff experiencing bullying, harassment or abuse from staff | 15.02% | 21.28% | 6.26% point disparity gap | 13.6% | 24.1% | 10.5% point disparity gap | The experience of white staff has deteriorated and returned to 2020 21 levels. The experience of BME staff has improved by 2.82% points and the disparity gap has decreased |
| % Staff believing organisation provides equal opportunities for career progression | 64.27% | 53.45% | 10.82% point disparity gap | 68.2% | 50.2% | 18% point disparity gap | There has been an improvement for BME staff but a decrease for white staff. Despite this, there is still a disparity between white and BME staff, although there has been a significant improvement this year |
| % Staff experiencing discrimination from manager, team lead or colleague | 5.53% | 15.57% | 10.04% point disparity gap | 4.8% | 17.3% | 12.5% point disparity gap | There has been an improvement for BM staff but a deterioration for white staff. Despite this, there remains a large disparity between white and BME staff however the disparity gap has improved over the last reporting period |
| % Trust’s Board membership compared to overall workforce | 85.71% | 14.29% (overall work-force is 11% BME) | BME Board Members averaged 10.6% across North East and Yorkshire. (2023 National WRES) | 92.3% | 7.7% (overall work force was 9.06% BM ) | BME Board Members averaged 9.3% across North east and Yorkshire. (2022 National WRE S) | The Trust Board is more representative than the overall BME workforce |
Key Findings
• BME staff make up 3% of the overall non-clinical workforce, yet 82.9% of BME staff are in band 5 or below. This is compared to 77.6% of white staff in band 5 or below.
• BME staff make up 10.9% of the overall clinical workforce, yet 79.3% of BME staff are in band 5 or below. This is compared to 46.5% of white staff in band 5 or below.
• Despite BME staff making up nearly half (49.2%) of the overall medical workforce, only 55.1% are at Consultant grade. This compares to 72.8% of white medical staff being at Consultant grade. White medical staff at Consultant grade increased by 16% points, and BME medical staff at Consultant grade increased by 12% points. There is a 17.7% point disparity between BME and white medical staff at Consultant grade (13.7% point disparity last year).
• The percentage of staff experiencing bullying, harassment or abuse from patients, relatives, or the public has marginally increased for BME staff, and marginally decreased for white staff. Despite marginal differences, the disparity gap between the experience of BME and white staff has widened to 11.85% points, the disparity last year was 9.6% points.
• The percentage of BME staff believing the organisation provides equal opportunities for career progression has increased by 3.25% points, however the result for white staff has deteriorated by 3.93% points. There is a 10.82% point disparity between BME and white staff according to the NHS Staff Survey 2023 (this gap was 18% in 2022).
Actions
• Continue work to address progression opportunities for staff as part of agreed Trust Equality Objectives.
• Relaunch Give Respect Get Respect in conjunction with a research study into the experience of bullying in collaboration with the National Institute for Health and Care Research and with the Trust Research Innovation and Clinical Effectiveness team. The study will be informed by evidence-based research and will propose interventions that will be designed to reduce incidences and disparity between experiences in relevant WRES Metrics.
• Introduce a campaign for ‘My Equality and Diversity’ reporting within the Electronic Staff Record (ESR). The aim of the campaign will be to encourage staff to update their ethnicity within ESR, which will also contribute towards data collection for race pay gap reporting.
• Establish an EDI dashboard and run quarterly checks on data to pinpoint any areas of concern.
• Relaunch the Cultural Ambassador programme and consider Cultural Ambassador involvement within recruitment processes.
Workforce Disability Equality Standard (WDES)
The most recent WRES and WDES Annual Report (2024/25) was published in August 2024. The data compiled within this report is from a snapshot taken on 31 March 2024, as well as findings from the most recent NHS Staff Survey which took place in Autumn 2023.
| Metric |
CNTW Figure for Latest Reporting period Disabled |
Non- Disabled | Comments |
CNTW Figures for Previous Reporting Period Disabled |
Non- Disabled | Comments | 2024 Trend |
|---|---|---|---|---|---|---|---|
| Overall workforce | 723 | 6601 | Disabled staff 8.9% of total workforce | 648 | 6334 | Disabled staff 8.2% of total workforce | Disabled workforce has increased |
| Non-Clinical Band 5 or below | 134 (85.9%) | 979(77.1%) | 10% of non-Clinical staff are disabled | 85.6% | 80.1% | 9% of non-Clinical staff are disabled | There are more non-clinical disabled staff at Band 5 or below than non-disabled staff |
| Clinical Band 5 or below | 267(49%) | 2495(49%) | 8.7% of Clinical staff are disabled | 50.9% | 48.1% | 8.1% of Clinical staff are disabled | The ratio of disabled and non disabled clinical staff is the same |
| Medical consultant grade | 12 (54.5%) | 154 (61.8%) | 3% of Medical staff are Disabled | 58.8% | 61.8% | 6.2% of Medical staff are Disabled | There are more non disabled staff at Consultant Grade |
| Staff Appointed from Shortlisting | 84 (600 short listed) | 933 (4766 shortlisted) | Non- disabled staff are more likely to be appointed from short listing (1.398) | 58 (647 short listed) | 680 (14022 short listed) | Disabled staff are more likely to be appointed from shortlisting (0.54) | Non disabled candidates are more likely to be appointed, compared to last year where disabled candidates were more likely to be appointed |
| Staff entering formal capability process | No figures available for 2024. | No figures available for 2023. | |||||
| % Staff experiencing bullying, harassment or abuse from patients, relatives or public | 28.26% | 24.39% | 3.87% point disparity gap | 30.5% | 25.7% | 4.8% point disparity gap | Improvement for disabled staff over the last 3 reporting periods. The disparity gap has also decreased |
| % Staff experiencing bullying, harassment or abuse from manager | 8.19% | 4.49% | 3.7% point disparity gap | 8.1% | 4% | 4.1% point disparity gap | The figures remain similar to the last reporting period, with a slight decrease in the disparity gap |
| % Staff experiencing bullying, harassment or abuse from colleagues | 16.77% | 10.42% | 6.35% point disparity gap | 15.8% | 9.5% | 6.3% point disparity gap | Slight increase for both disabled staff and non disabled staff |
| % Staff or colleagues reporting bullying, harassment or abuse at work | 65.26% | 71.96% | 6.7% point disparity gap in favour of disabled staff | 71.8% | 70.1% | 1.7% point disparity gap | Fairly significant decrease for disabled staff and disparity gap in favour of disabled staff |
| % Staff believing organisation provides equal opportunities for career progression | 59.98% | 65.03% | 5.05% point disparity gap | 63.7% | 61.6% | 2.1% point disparity gap | Fairly significant decrease for disabled staff, with slight improvement for non disabled staff. The disparity gap has widened |
| % Staff who felt pressure from manager to work , despite not feeling well enough | 17.27% | 10.23% | 7.04% point disparity gap | 18.1% | 11% | 7.1% point disparity gap | Improvement for both disabled and non disabled staff. the disparity gap remains around 7% |
| % Staff satisfied with extent that Organisation values their work | 44.08% | 51.76% | 7.68% point disparity gap | 44.6% | 54.1% | 9.5% point disparity gap | Slight decrease for both disabled and non disabled staff, however the disparity gap has improved |
| % Staff with long-lasting health condition or illness saying employer has made adequate adjustment (s) to carry out their work | 81.04% | N/A | 81.9% | N/A | Slight decrease following an improvement in 20 21 and 21 22 reporting periods. The figure has remained around 81% for the past three years | ||
| % Trust’s Board Membership Compared to Overall Work force | 7.1% | 92.9% | Compares with 8.9% overall Disabled workforce | 7.1% | 92.9% | Compares with 8.2% overall Disabled workforce |
Key Findings
• The number of disabled applicants appointed from shortlisting has increased by 45% this year, with an increase of 37% for non-disabled applicants.
• Shortlisting of disabled applicants decreased by 3% this year and increased by 29% for non-disabled applicants.
• Disabled staff make up 10% of the overall non-clinical workforce, yet 85.9% of disabled non-clinical staff are in band 5 or below. This is compared to 77.1% non-disabled staff being in band 5 or below. The disparity between disabled and non-disabled staff at band 5 or below has increased from 5.5% points to 8.8% points compared to last year.
• Disabled staff make up 3% of the overall medical workforce and 54.5% are at Consultant Grade. This compares to 61.8% of non-disabled staff and therefore there are more non-disabled staff at Consultant Grade than disabled staff. The disparity between disabled and non-disabled staff at Consultant grade has increased from 3% points to 7.3% points compared to last year.
• There has been a marginal increase in both disabled and non-disabled staff experiencing bullying, harassment or abuse from colleagues. The disparity between the experience of disabled and non-disabled staff remains around 6.3% points.
• According to the NHS Staff Survey 2023, there has been a significant decrease in the reporting of bullying, harassment or abuse at work for disabled staff. There is a 6.7% point disparity between disabled and non-disabled staff with non-disabled staff reporting higher levels of bullying, harassment or abuse at work.
• According to the NHS Staff Survey 2023, the number of disabled staff believing the organisation provides equal opportunities for career progression has decreased by 3.72% points, while increasing by 3.43% points for non-disabled staff. The disparity gap has widened.
• The NHS Staff Survey 2023 reported that there was a slight decrease for both disabled and non-disabled staff being satisfied with the extent the organisation values their work, however the disparity gap has improved.
• The percentage of disabled staff reporting in the NHS Staff Survey that the organisation has made adequate adjustments to carry out their work has remained around 81% for the last three reporting periods.
Actions
• Continue work to address progression opportunities for staff as part of agreed Trust Equality Objectives.
• Relaunch Give Respect Get Respect in conjunction with a research study into the experience of bullying in collaboration with the National Institute for Health and Care Research and with the Trust Research Innovation and Clinical Effectiveness team. The study will be informed by evidence-based research and will propose interventions that will be designed to reduce incidences and disparity between experiences in relevant WDES Metrics.
• Introduce a campaign for ‘My Equality and Diversity’ reporting within the Electronic Staff Record (ESR). The aim of the campaign will be to encourage staff to update their disability status within ESR, which will also contribute towards data collection for disability pay gap reporting.
• Establish an EDI dashboard and run quarterly checks on data to pinpoint any areas of concern.
• Measure the impact of the Reasonable Adjustments Toolkits for Managers and Staff.
• Work towards becoming a level 3 (highest level) Disability Confident Employer. Work to take place in conjunction with Disabled Staff Network and to be completed before the next Disability Confident validation in 2026.
Workforce Bullying Evaluation
The Trust’s Board of Directors agreed three core Equality, Diversity and Inclusion objectives in November 2023. One of these objectives is to address experiences of bullying in the workplace. The Workforce Race and Disability Equality Standard annual report was presented to EMG in June 2024 which included a number of recommendations, including an action to relaunch the Give Respect Get Respect campaign. As part of the relaunch, an opportunity arose to collaborate with the Directorate of Research Innovation and Clinical Effectiveness alongside a research associate from the National Institute for Health and Care Research to evaluate staff experiences of bullying. The survey was designed to focus solely on bullying.
This differs from the National NHS Staff Survey which combines bullying, harassment, and abuse into one question. It was agreed to include a clear definition of what behaviours amount to bullying as this is something that is not defined in the national survey. The survey ran over Sept-Aug 2024 over 3000 staff completed the survey with many insights and themes emerging from the analysis.
Round table discussions of these themes took place in December 2024 with Executive directors and the Trust Leadership Forum – where the Trust’s senior leaders come together to discuss key initiatives and priorities.
The Equality, Diversity and Inclusion Team continue to engage with our Senior Leaders, Staff Networks and research colleagues to ensure these important discussions continue to take place.
Reasonable Adjustments Toolkit for Staff and Managers
To keep supporting disabled staff, last year the Trust began work to develop a set of resources to help disabled staff and their managers with the process of making reasonable adjustments at work. Officially launched 13 May 2024 during NHS Employers Equality, Diversity and Human Rights Week.
These toolkits make it clear how to ask for help, what managers need to do, and where to get more advice. To develop them, we held meetings with staff, worked in focus groups, and got feedback through different forums.
Our goal was to make sure the toolkits fit with the law and our own Trust values of equality. It is vital that we make sure our staff get what they need to help them carry out their work comfortably, safely, and effectively. Not only is this our legal duty and important for people’s own wellbeing, but it also helps us to retain staff.
As well as a toolkit with advice for disabled staff, we developed a toolkit specifically for managers, because we felt it was important to make sure managers know what they need to do when someone asks for help. Mangers must support their team members, both during and after making these changes.
Choices College
Choices College (formerly Project Choice) is a specialist College providing tailored educational support, and a supported internship course for young adults aged 16-24 who are autistic and/or have learning difficulties/disabilities.
This is a partnership programme, which means that Choices College support coaches and coordinators ensure the students are well supported throughout their internship. Teams who accepted placements were offered mentor training (tailored to the students they hosted) as well as ongoing support from Choices College area managers.
New Trauma-Informed Health, Wellbeing and Attendance Policy
CNTW’s new Health, Wellbeing and Attendance Policy went live in March 2025. This replaces the Managing Sickness Absence Policy. The new policy was written in collaboration with a broad range of colleagues across the Trust, including Workforce and Organisational Development and the Disabled Staff Network.
It is the first workforce policy to be written through a trauma-informed lens. To deliver trauma-informed services to our patients, it’s important to support our staff using the same principles.
Staff Networks
The Trust has four Staff Networks: Cultural Diversity Staff Network, Disabled Staff Network, LGBT+ Staff Network and Armed Forces and Veterans Network. Each network has two co-chairs who meet regularly with the Equality, Diversity and Inclusion Team to talk about cross-cutting issues as well as attend Trust Leadership Forums. Each staff network is allocated an annual budget for initiatives that will support key work to address Trust wide actions, as well as weekly protected release time for each co-chair to undertake network duties. The following sections provide highlights of staff network activities during 2024/25:
Cultural Diversity Staff Network
The Cultural Diversity Staff Network actively engages and contributes ensuring equality, acceptance and inclusion within the Trust. Notable events hosted by the network this year:
•Cultural Diversity Network Book Club
•Black History Month – Reclaiming the Narrative
o Virtual event with guest speakers from CNTW’s workforce
o Themes menus in Trust cafés
o History, arts, and healthcare exhibition event
o Wear Red Day
• South Asian Heritage Month
o Virtual event with guest speakers from staff in different professions who are from South Asian backgrounds
Disabled Staff Network
Committed to creating a fair and diverse workplace. The staff network actively engages and contributes towards ensuring equality, acceptance and inclusion within the Trust. Notable events hosted by the network this year:
•Disability History Month Ableism Campaign and Lunch and Learn Sessions
o Internalised Ableism & I
o Unlearning Ableism
o Let’s Talk About Ableism
o Ableism – Everyone’s Business
o The Autistic Advocate
o Disability Rights
o Disability and Reasonable Adjustments
LGBT+ Staff Network
The aim of the LGBTQ+ Staff Network is to promote a working environment where all LGBT+ staff feel supported, valued, and to challenge discrimination. Notable events hosted by the network this year:
• LGBT+ History Month
o LGBT+ and Medicine
o Gender: Past, Present and Future
o LGBT+ Over the Years
o Neuro Diversity and the LGBT+
• Trans Day of Remembrance
• Pride
o Pride Party Packs and resources
o ‘Our Authentic Selves’ video campaign
Armed Forces and Veterans Network
The group aims to ensure the Trust provides support to staff who are connected with the armed forces. It is key to helping the Trust fulfil its duties under the Armed Forces Covenant and the requirements of being a Veterans Aware organisation. CNTW is accredited as a Veteran Aware Trust and holds a Gold Award under the Defence Employer Recognition Scheme. Notable events hosted by the network this year:
• Armistice Day
o Breakfast club event
o Chapel service
• Armed Forces Day – Gregg Stephenson’s story
Gender Pay Gap
The gender pay gap shows the difference in the average pay between all men and women in the workplace. This is different to equal pay. Equal pay deals with the pay differences between men and women who carry out the same jobs, similar jobs, or work of equal value. This report fulfils the Trust’s legislative requirements and sets out what the Trust is doing to close the gender pay gap. The figures for the 6 metrics we are required to report on for 2023/24 (based on 31 March 2024 snapshot) are as follows:
• Mean gender pay gap is 9.90% - a decrease of 1.66% points on 2022/23.
• Median gender pay gap is - (minus) 2.29% - This indicates that the median hourly rate of pay for women (£17.16) is now greater than for men (£16.78).
• Percentage of men receiving bonus pay is 1.47% (2.0% previous year) and women 0.36% (0.5% previous year).
• Mean (average) gender pay gap using bonus pay is 11.88% - up from 10.99% in 2022/23.
• Median gender pay gap using bonus pay is 45.77% up from 39.35% in 2022/23.
• Percentage of men and women in each hourly pay quartile.
• Percentage of men and women in each hourly pay quartile
|
CNTW Figures 0f 2023-2024 Male |
Female |
CNTW Figures of 2022-2023
Male |
Female |
CNTW Figures for 2021-2022
Male |
Female |
|
|---|---|---|---|---|---|---|
| Top quartile | 27.08% | 72.92% | 26.83% | 73.17% | 27.7% | 72.3% |
| Upper middle | 20.40% | 79.60% | 19.79% | 80.21% | 20.0% | 80.0% |
| Lower middle | 27.05% | 72.95% | 26.03% | 73.97% | 27.4% | 72.6% |
| Lower quartile | 22.91% | 77.09% | 20.84% | 79.16% | 19.3% | 80.7% |
Actions taken to close the gender pay gap
Commitment to paying the UK Living Wage: the Trust became an accredited Living Wage Employer in 2013.
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust was the first NHS Trust in the North East of England to accredit with the Living Wage Foundation and have continued to champion the Living Wage during Living Wage Week each November. The Real Living Wage is worked out independently and takes into account rising bills and costs. Paying a Living Wage means that all staff are appointed on at least Band 2 of the Agenda for Change pay scales for NHS staff.
Encouraging flexible working: the Trust promotes a supportive and flexible working culture. We recognise that flexible working helps employees to achieve a better balance between their work and home life, as well as improve service delivery through a flexible workforce. It can help the Trust become an employer of choice, aid recruitment and retention, reduce sickness absence and improve employee engagement, leading to an improved patient experience.
Inclusive recruitment: the Trust has undertaken a substantial piece of work examining our recruitment processes, with the objective of removing any barriers to entry by protected characteristics as defined by the Equality Act 2010. Many of the measures we have adopted have recently been implemented. The next key piece of work that follows on from this will be a review of job descriptions. As part of this we will carefully examine and remove any gender bias that may affect the numbers of men and women applying for jobs with the Trust.
Continue with Springboard for Women Programme: across society, the NHS, and here in the Trust, people who identify as having a protected characteristic tell us they do not always have the same opportunities as others to learn, develop and progress. Springboard for Women, one of several development programmes offered by Springboard Consultancy, provides women with the inspiration, tools and confidence boost to enable them to choose what they want to do and to take their next steps (at work, in life) when the time is right for them.
Future actions to close the gender pay gap
Mend the Gap Recommendations: we will in 2025/26 continue to address the actions against Mend the Gap report to ensure that we are doing all we can to address pay gaps for Doctors.
Address Intersectional Issues: as part of our response to the EDI Improvement Plan, we will produce our first Race Pay Gap report and will begin to collect data to look at the gaps for other protected characteristics. We will compare the results of these to the Gender Pay Gap and examine if there are intersectional issues which we need to address. Such work will also help inform our key EDI objective of progression for staff who share protected characteristics. We will triangulate these results with the Gender Pay Gap and figures for our other mandatory Equality and Diversity Workforce Reports.
Staff Survey 2024
The annual staff survey opened on 30 September 2024 and closed on 29 November 2024, an eight-week period for completion. There were 7950 members of staff were eligible to take part in the survey, 3354 staff completed the survey giving an overall response rate of 42%. There is a communications and engagement plan to promote the survey across the Trust which included virtual sessions, infographics, and the sharing of examples of where staff survey feedback had instigated a change.
This is the second consecutive year that the NHS Staff Survey has been opened to bank workers. There were 101 workers who took part in the survey providing an overall response rate of 22% of the bank workforce. This is an improvement to the response rate from the 2023 survey of 20%.
For 2024 we opted for a mixed mode method for completion of the staff survey. Our Inpatient services received a paper survey, and all others received an electronic survey, whereby all staff received an email with a dedicated link to their individual survey. This was to support our ward-based staff who do not have easy access to their emails to complete the survey.
The 2024 response rate is up by 1 percentage point on our response rate of 41% in 2023. The 2024 median response rate for Mental Health and Learning Disability Trusts was 54%.
This is the fourth consecutive year that we have a below average response rate. Our highest was 2018 when our response rate was 66.5%, the highest response rate in our comparator group.
| Response Rate | 2021 | 2022 | 2023 | 2024 |
|---|---|---|---|---|
| Trust | 45% | 47% | 41% | 42% |
| National Average (Mental Health/Learning Disability) | 52% | 50% | 52% | 54% |
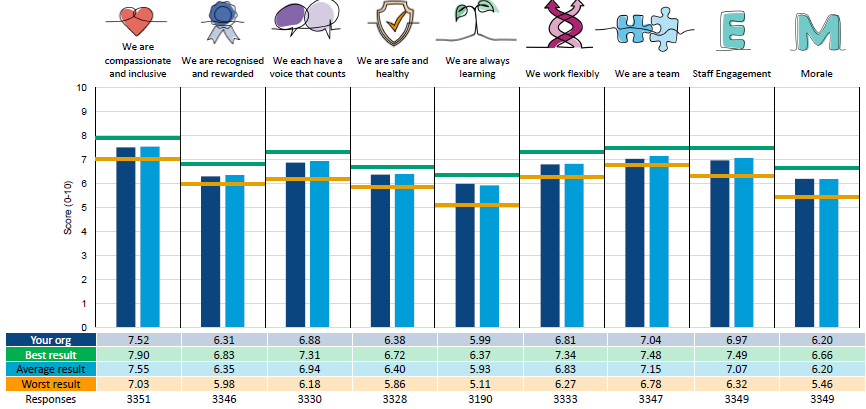
2024/2023, 2023/22 and 2022/21
Scored for each indicator together with that of the survey benchmarking group (mental health and learning disability Trusts) are presented in the table below. (Note: the 2023/24 results reflect the feedback gathered from the most recent staff survey undertaken Autumn 2024).
| Staff Survey comparison indicators (People Promise elements and themes) |
2023/24
Trust Score |
Benchmarking Group Score |
2022/23
Trust Score |
Benchmarking Group Score |
2021/22
Trust Score |
Benchmarking Group Score |
|---|---|---|---|---|---|---|
| People Promise: | ||||||
| We are compassionate and inclusive | 7.63 | 7.58 | 7.7 | 7.5 | 7.9 | 7.5 |
| We are recognised and rewarded | 6.44 | 6.41 | 6.4 | 6.3 | 6.8 | 6.3 |
| We each have a voice that counts | 7.03 | 7.01 | 7.2 | 7.0 | 7.4 | 7.0 |
| We are safe and healthy | 6.44 | 6.38 | 6.5 | 6.2 | 6.6 | 6.2 |
| We are always learning | 6.03 | 5.93 | 6.0 | 5.7 | 6.1 | 5.6 |
| We work flexibly | 6.86 | 6.84 | 6.8 | 6.7 | 7.1 | 6.7 |
| We are a team | 7.15 | 7.18 | 7.2 | 7.1 | 7.4 | 7.1 |
| Staff engagement | 7.09 | 7.11 | 7.2 | 7.0 | 7.4 | 7.0 |
| Morale | 6.23 | 6.17 | 6.3 | 6.0 | 6.5 | 6.0 |
Respectful Resolution
The Respect Campaign was rolled out across the Trust, following ‘Train the Trainer’ workshops from A Kind Life in 2021. The programme provides helpful tools and guides staff through the process of developing team values, reflecting on and identifying behaviours, initiating respectful conversations, and supporting resolution with colleagues.
The goal is for teams to create a ‘safe space’ culture and to reduce the need for formal processes. A suite of resources continues to be accessed by staff which are available online. This toolkit also underpins the Trusts new resolution policy.
Organisational Improvement/Development
To help CNTW balance the daily challenges of increased service demands, rising expectations and a testing financial position, whilst delivering significant transformation work, several key areas of development were progressed during 2024/25 and will continue into 2025/26.
Clinical Support Worker Leadership Development Programme
The Trust is committed to devising and launching a modular Clinical Support Worker (CSW) Leadership Development Programme Offer extending beyond the supernumerary HCSW Induction week. Contribution from CSWs is essential to inform, and influence content, to obtain views and feedback around subject areas held as important to the CSW role, relevant for personal and professional growth, career development and, as a potential platform, to further opportunities within the Trust.
Developing Leadership and Management capacity and capability
The Messenger Report 2022, rightly points out the gaps in developing and supporting leaders, it states investing in developing leadership and management capacity and capability, to enable a motivated, valued, collaborative, inclusive, resilient workforce, is the key to better outcomes and should sit alongside other operational and political priorities.
The Trust is ensuring leadership and management development is strategically aligned to delivery of Trust Strategy, ambitions, commitments, and values.
The Trust continues to offer development opportunities, such as, the NHS Mary Seacole Programme, Medical Leadership CPD, International Fellows Leadership Development, leadership development via the Apprenticeship Framework, and participation in the NHS Graduate Management Training Scheme. Other developments include:
• Management Development – a suite of programmes has been developed and being rolled out to ensure managers are confident and capable to lead and direct the efforts of others, facilitate healthy and well teams, apply in-depth knowledge and expertise and make effective decisions.
• (Future) Young Leaders – Dream Placements Programme – the North Cumbria Locality participates in this Cumbria initiative, managed by the Centre for Leadership Performance. The initiative brings together motivated students aged 16-18 with successful organisations in a programme that provides a week’s Dream Placement, for young people. The programme enables the Locality to connect with its potential future workforce and showcase the breadth and depth of opportunities available in CNTW and
the wider health and care system.
People systems and processes
Aligning people and people management systems to strategy continues to be a focus for CNTW. In addition to ongoing work such as strengthening partnership working with Trade Unions and wider partners, developing more inclusive recruitment, implementing the Allocate healthcare roster system that enables multidisciplinary rostering, implementing the Electronic Staff Record as the Trust’s single workforce information system, and the adoption of the Patient Safety Incident Reporting Framework that enables compassionate engagement and involvement of those affected by patient safety incidents, other examples of work done in the year includes:
• Inclusive Mentoring - evaluation of a pilot programme which aimed to promote wider cultural change/transformation to facilitate a culture of inclusion was concluded. The pilot focused on building cultural awareness and diversity through mentoring relationships between Staff Network members and Non-Executive and Executive Directors. Developing, supporting, and enabling teams – there is compelling evidence to show that investing in teams develops a culture that delivers high quality, compassionate, inclusive care. Such a culture is enabled through team leaders/managers and colleagues creating a climate which ensures clarity on what is expected from the team, and everyone working in it. It builds trust and camaraderie and high levels of skill to do their job well, and to thrive.
• Working with teams, is a priority for the organisation and in the past twelve months many teams have been supported to; imagine and inform the future shape of their service/care, improve quality, establish new and different ways of working, strengthen interprofessional relationships and improve decisions making.
• Coaching – the Trust continues to invest in coaching as a means of developing its people and the organisations effectiveness. The launch of a new Coaching request capacity on the Trust Intranet, has allowed staff to take ownership of whom they access for coaching, whilst still being overseen via Trust Lead on coaching. The coaching network is supported by Trust lead and meet bi-monthly as well as receiving group and individual supervision. All coaches are CMI Level 5 qualified. This supports recruitment of new and “rewarding” long serving Coaches, which is important as they coach on a voluntary basis. Typically, Coaches provide support for staff working through issues associated with; decision making, ability to deal with change, career development, working in a new team, and interprofessional/interpersonal relationships.
This framework professionalises HR and will support development of the Trust’s workforce and organisational development function in line with ‘With You in Mind’, including enabling development of a workforce and organisational development career pathway.
Staff engagement
There is a range of interventions in place including engaging staff in development of ‘With You in Mind’, events to engage staff and others in our core transformation work, bespoke focus groups and forums exploring current issues such as development of quality priorities, exploring generational workforce needs and staff survey conversations and action planning. Continuation of previously implemented new approaches with the aim of elevating and embedding staff engagement more formally across the Trust. We have continued with the Chief Executive message, Executive Team Live Q&A, fortnightly manager’s forum.
Employee Consultation
We continue to value the strong working relationships we have developed with our staff side representatives. We continue to have both informal and formal meetings with staff side colleagues both within the Trust and at a regional level. Trade Union Management Forum and Local Negotiating Committee remain the forums to discuss key Trust wide and strategic issues with trade union representatives. Staff side representatives play a crucial role in promoting good employee relations and supporting effective change management, as well as assisting in the training and development of staff, conducting work relating to health and safety and involvement in other key pieces of work such as assisting in the areas of work relating to the Equality Act.
The Trust has several policies which allow staff to raise any matters of concern, and we run management skills training to equip managers to support staff with these policies. These include:
• Resolution Policy CNTW (HR) 05
• Freedom to Speak Up CNTW(HR)06
• Handling Concerns about Doctors CNTW(HR)02
• Dignity and Respect at Work CNTW (HR)08
The Trust has developed an HR framework agreed with Staff Side which focusses on how we will engage and consult with staff during organisational change. Whilst we are not legally required to undertake formal consultation for much of the organisational change the Trust has agreed it will still utilise a consultation process approach. During 2024/25 specific consultations with staff have included the following:
Secure Care Group
•Provision of a Secure pool
North Community
• Northumberland Emotional Wellbeing Support Team (NEWST) – change of base
• North Cumbria Single Point of Access Call Handlers – change of shift pattern
• South Community Treatment Team - restructure
• North Cumbria Crisis Team - change of base
Inpatient Care Group
• Temporary closure of Bede Ward for urgent estates work
• Permanent closure of Bede Ward
• Reprovision of mental adult acute service in West Cumbria
Corporate
• Audit 1 Office moves and Senior Manager structure
• Patient Carer – restructure
• Safer Care – restructure
• Trust Innovation – restructure
• Workforce Development – restructure
Involvement of staff in our Foundation Trust’s performance
The Trust is committed to fully involving all our staff in taking an active role and interest in the quality and performance of our services. A detailed performance report is prepared monthly for the Board of Directors, Executive Management Team, senior managers and clinical leaders.
The continued development of the performance dashboards has enabled managers to easily access a wide range of performance information relating to their teams, and staff can access their own personal information in ‘my dashboard’ relating to, for e ample, training records and absence history.
Raising Concerns Policy
In Sir Robert Francis’ Freedom to Speak Up review it stated that not all concerns raised become subject to formal investigation under Raising Concerns or Grievance Policies. This is an approach welcomed and adopted by the Trust.
The Trust has adopted the national policy which is available on the Intranet and has been communicated to all staff. The Trust has four Freedom to Speak up Guardians (FTSUGs) who are undertaking the role jointly and have done so since January 2025. Previously there were two FTSUGs whose tenure ended in December 2024. Each of the four FTSUGs have one day per week allocated to their FTSUG role. They continue to actively recruit and support the FTSU Champions, raise the profile of the importance of speaking up, as well as supporting individual cases.
The Guardians have sought to help staff resolve issues themselves without the Guardians having to escalate the issue. This may be through encouraging conversations to take place with managers, signposting staff to utilise existing processes and support mechanisms available or providing some confidence and reassurance to staff.
During the past year 117 issues have been raised either centrally, CQC or with the FTSUGs. All concerns are encouraged to be resolved through the utilisation of local policies and procedures. However, where the FTSUGs feel there is a wider concern this may be escalated to director level. Concerns are dealt with to look for a resolution to the problem as well as identifying and learning and disseminating the learning as appropriate. Feedback is provided to individuals who have been involved in raising the concern.
Trade Union Facility Time
Trade Union (Facility Time Publication Requirements) Regulations 2017 were introduced in April 2017 and require Public Sector employers to publish the total costs of paid facility time taken by employees who are trade union officials. The period runs from 1 April to 31 March each year.
The published information is also meant to differentiate between statutory facility time (where representatives have the right to paid time off) and non-statutory facility time. Information must be published on the Trust's website before 31 July; on a government website; and be included within the Annual Report.
This is the seventh report and covers the period 1 April 2024 to 31 March 2025. It will also draw comparison with the previous six years reporting. Information that must be published is:
• The total number of employees who were relevant union officials during the period.
• The percentage of each of these employees' working time spent on facility time.
• The percentage of the employer's total pay bill spent on facility time.
• Time spent on paid trade union activities as a percentage of the total paid facility time hours.
For the purpose of the Act, statutory facility time is defined as:
• Negotiating pay, terms and conditions
• Helping members with disciplinary or grievance procedures including meetings to hear their cases
• Accompanying union members to attend meetings with line managers to discuss some employment related issues were deemed appropriate working requests
• Participate in Agenda for Change job evaluation panels
• Discussing issues that affect union members, e.g. redundancies
Union Learning Representatives also have the right to paid time off to:
• Analyse the learning and training needs of union members
• Give information and advice about learning or training
o Arrange and encourage learning or training
o Discuss their activities as a Learning Representative with their employer
o Train as a Learning Representative
Similarly, Health and Safety activities are also regarded as statutory activities. The Act also requires the reporting of paid time off for non-statutory activities; this includes:
• Attendance at union meetings
• Going to meetings with union officials
• Union training
| 2024-25 | 2023-24 | 2022-23 | 2021-22 | 2020-21 | 2019-20 | 2018-19 | 2017-18 |
|---|---|---|---|---|---|---|---|
| £208,808 | £231,369 | £228,543 | £210,611 | £212,975 | £125,194 | £133,627 | £119,232 |
Table 10: Employee Expenses and Employee Numbers for the period 1 April 2024 – 31 March 2025
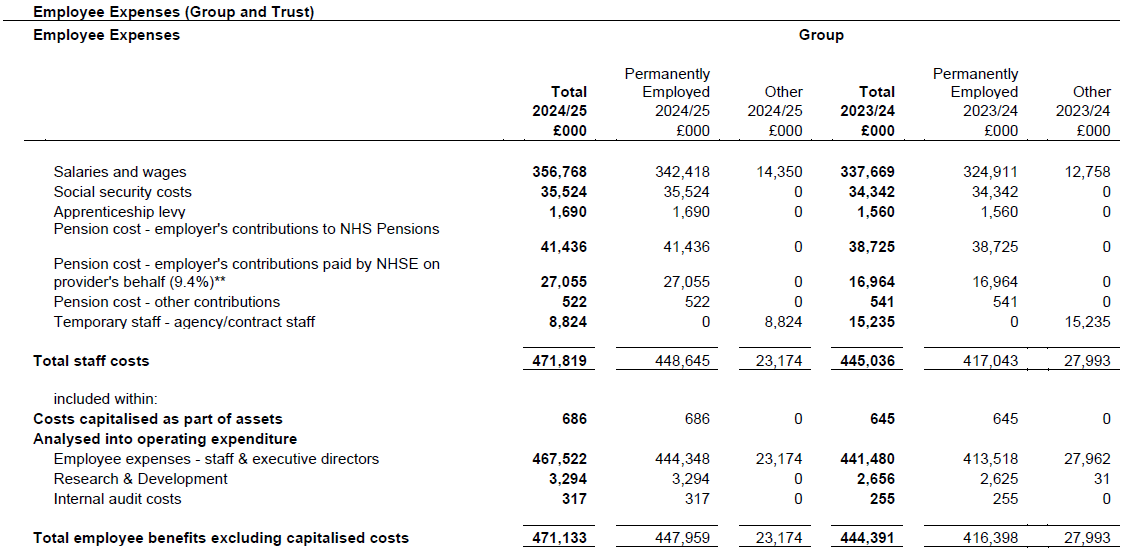
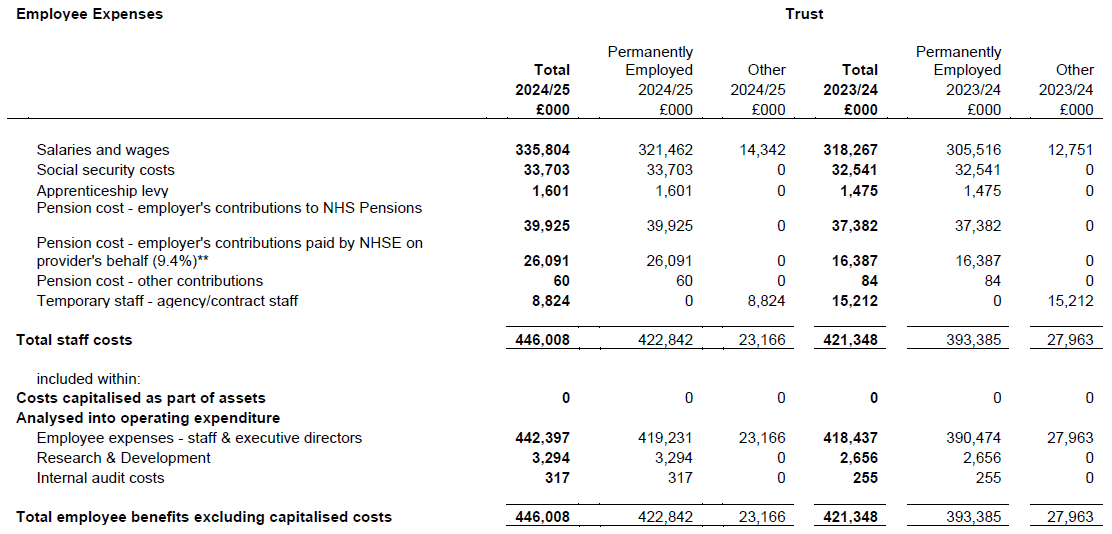
**See note 3.1 for Pension cost - employer's contributions paid by NHSE on provider's behalf (9.4% for month 12 only), (2023/24 was 6.3%)
Expenditure on Consultancy
The Trust expenditure on consultancy during 2024/25 is provided within the Annual Accounts.
Off-Payroll Engagements – CNTW Group
The Trusts policy for off payroll engagements is to reduce these wherever possible, this is done by engagement with the acquiring service and the identified staff to transfer these to on-payroll arrangements. These types of transactions range from consultancy, training, workshops, webinars, and assessments. there have been no penalties incurred due to non-compliance of off payroll worker legislation.
Table 11 Off payroll engagements (CNTW Group)
Highly paid off payroll worker engagements as of 31 March 2025, earning £245 per day or greater
| Number of existing engagements as of 31 March 2025 | 0 |
|---|---|
| Of which... | 0 |
| Number that have existed for less than one year at time of reporting | 0 |
| Number that have existed for between one and two years at time of reporting | 0 |
| Number that have existed for between two and three years at time of reporting | 0 |
| Number that have existed for between three and four years at time of reporting | 0 |
| Number that have existed for four or more years at time of reporting | 0 |
All of the off payroll arrangements relating to Medics operating on a self employment basis through Personal Services Companies (PSCs) and through Stafflow are now on payroll arrangements following the implementation of IR35.
Highly paid off payroll workers engaged at any point during the year ended 31 March 2025 earning £245 per day or greater.
| Number of off-payroll workers engaged during the year ended 31 March 2025 | 14 |
|---|---|
| Of which... | 0 |
| Not subject to off-payroll legislation* | 0 |
| Subject to off-payroll legislation and determined as in-scope of IR35* | 7 |
| Subject to off-payroll legislation and determined as out-of-scope of IR35* | 7 |
| Number of engagements reassessed for compliance or assurance purposes during the year | 0 |
| Of which: number of engagements that saw a change to IR35 status following review | 0 |
* A worker that provides their services through their own limited company or another type of intermediary to the client will be subject to off payroll legislation and the Trust must undertake an assessment to determine whether that worker is in scope of intermediaries’ legislation (IR35) or out of scope for tax purposes.
Number of New Off-Pay roll Engagements of Board embers or Senior Officials with significant financial responsibility between 1 April 2024 – 31 March 2025
Number of off-payroll engagements of Board members or senior officials with significant financial responsibility, during the financial year - 0
Number of individuals that have been deemed ‘board members and/or senior officials with significant financial responsibility ’ during the financial year. This figure includes both off-pay roll arrangements and on-pay roll engagements - 0
Table 12: Exit Packages from the CNTW Group in 2024/25 and 2023/24
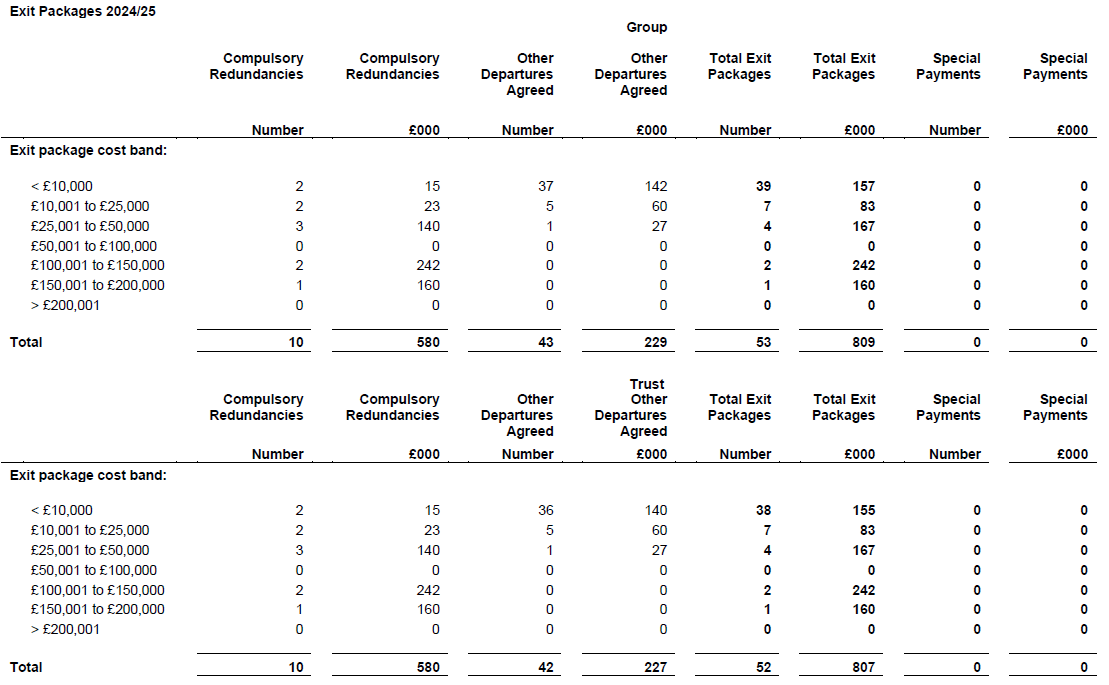
All redundancy and other departure costs have been paid within the provisions of Agenda for Change terms and conditions. The termination benefits included in exit packages relate to redundancy and early retirement contractual costs. There were no non-contractual payments made during the year.
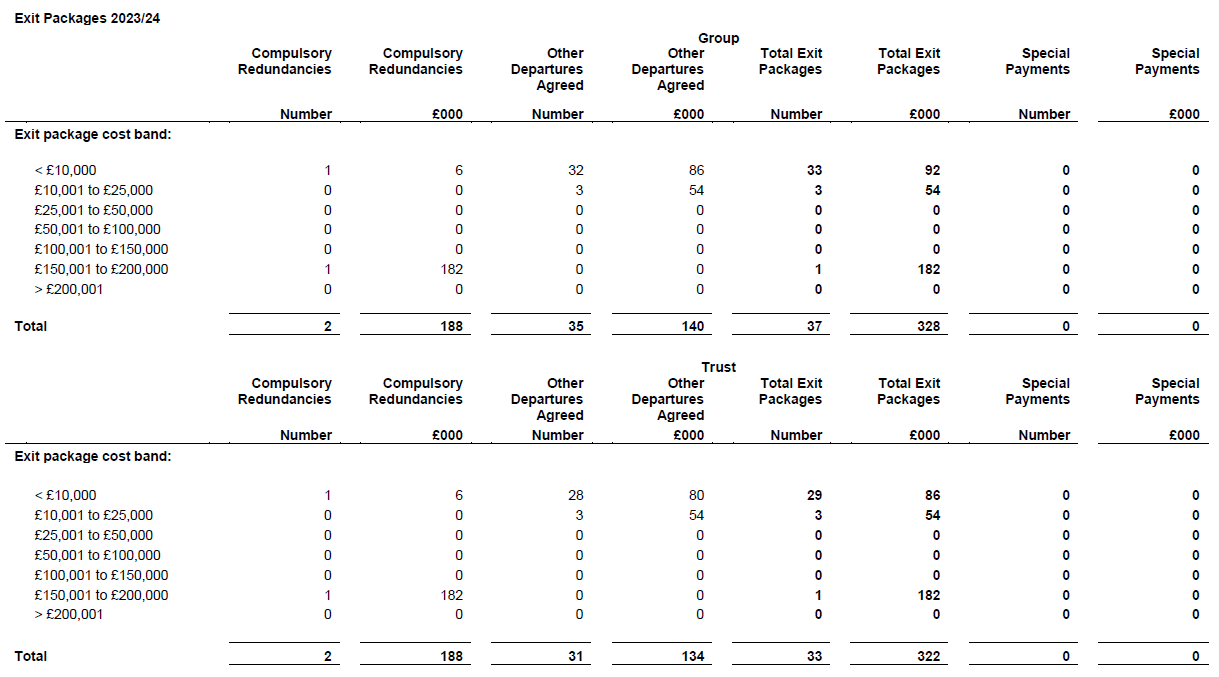
All redundancy and other departure costs have been paid within the provisions of Agenda for Change terms and conditions. The termination benefits included in exit packages relate to redundancy and early retirement contractual costs. There were no non-contractual payments made during the year.
Introduction
The Audit Committee provides an independent and objective review of our internal controls. It seeks high level assurance on the effectiveness of the Trusts governance (corporate and clinical), risk management and systems of internal control. It reports to the Board of Directors on its level of assurance.
The committee receives assurance from the Executive Team and other areas of the organisation through assurance reports and presentation updates, both regular and bespoke. It validates the information receives through the work of internal audit, e ternal audit and counter fraud. Assurance is also brought to the committee through the knowledge that Non Executive Directors gain from other areas of their work, not least their own specialist areas of expertise, attending Board and Council of Governors’ meetings, leadership visits and talking to staff.
Should our e ternal auditors (Mazars) carry out any non audit work Audit Committee has responsibility for ensuring that their independence is maintained. The committee will do this by reviewing and approving the scope of the work and the fees charged prior to the work being undertaken. The Council of Governors appoint the ternal Auditors and receive continual assurance by the inclusion of Governors as attendees at meetings of the Audit Committee.
The substantive membership of the Audit Committee is made up of three Non Executive Directors. The Chair of the Trust may not be a substantive member of the Committee. The Chief Executive attends one meeting during the financial year to present the Trust Annual Governance Statement. Other non Executive directors may be invited to attend on an ad hoc basis, either when it is deemed appropriate for other non executive directors to attend for a particular agenda item or to ensure quoracy.
Terms of Reference for the Audit Committee
The terms of reference for the Audit Committee were last ratified by the Board of Directors in June 2024. The terms of reference are reviewed each year in line with the annual reporting process and will be further reviewed at the April 2025 meeting of the Board.
The committee also carried out a review of its effectiveness in March 2025 in line with the requirements and guidance of the newly published NHS Audit Committee Handbook, March 2024. The feedback was very positive in most areas which cover composition, establishment and duties, compliance with legislation and regulation, internal control and risk management, internal audit, counter fraud and annual accounts and disclosure statements. The results were collated and then presented to the Committee at the April 2025 meeting. It was concluded that there was a high level of effectiveness of the committee and that there were no areas of concern.
Membership of the Committee and attendance at meetings
Membership of the Audit Committee is comprised of three Non Executive Directors. David Arthur was appointed as Chair of the Audit Committee on 14 January 2019 and stood down from his role on 13 January 2025. David Arthur’s successor, Robin Earl, Non Executive Director commenced in his role 1 July 2024 which provided enough time shadowing the role of Chair of Audit Committee taking up this position in January 2025. The Board is satisfied that the Chair of the Audit Committee has recent and relevant financial experience. All Non Executive Directors are considered to be independent.
As David Arthur, Non Executive Director also fulfilled the role of Senior Independent Director with the Trust declaring an ‘e plain’ position in the 2023/24 Annual Report, Michael Robinson Non Executive Director agreed to take on the role of Senior Independent Director between January and September 2025, it was therefore agreed Michael Robinson would e it the Audit Committee membership and Vikas Kumar will join as Non Executive Director from May 2025 which in turn provides a ‘comply’ approach to the Code of Governance.
In addition to the Non Executive Directors, the Executive Finance Director, Director of Communications and Corporate Affairs, Corporate Governance Manager/Deputy Trust Secretary, Managing Director of NTW Solutions Limited, ternal Audit and Internal Audit, including Counter Fraud, were all invited to each meeting during the year. Two Governor Representatives also attend meetings of the Audit Committee.
The table below shows attendance for members of the committee for the period 1st April 2024 to 31 March 2025.
| Committee member |
Audit Committee meeting dates 2024/25 08/05/24 |
19/06/24 | 07/08/24 | 06/11/24 | 06/12/24 | 14/01/25 | 04/02/25 |
|---|---|---|---|---|---|---|---|
| David Arthur, Chair – Non Executive Director | Y | Y | Y | Y | Y | - | - |
| Robin Earl – Non Executive Director (shadowing) | - | - | Y | Y | Y | Y | Y |
| Vikas Kumar, Non Executive Director | Y | N | Y | Y | Y | Y | Y |
| Brendan Hill, Non Executive Director | Y | Y | Y | Y | Y | Y | Y |
| Members in attendance |
Audit Committee meeting dates 2024/25 08/05/24 |
19/06/24 | 07/08/24 | 06/11/24 | 06/12/24 | 14/01/25 | 04/02/25 |
|---|---|---|---|---|---|---|---|
| Kevin Scollay, Executive Finance Director | Y | Y | Y | Y | Y | N | Y |
| Debbie Henderson, Director of Communications and Corporate Affairs | Y | Y | Y | Y | Y | Y | N |
| Kirsty Allan, Corporate Governance Manager/Deputy Trust Secretary | Y | Y | Y | Y | Y | N | Y |
| Tracey Sopp, Managing Director NTW Solutions Management **Representative Shaun Dixon Head of Accounting and Processing and Amy Gowans, Financial Accountant |
Y | Y | Y | Y | Y | Y** | Y |
| Internal Audit representatives (Helen Stephenson, Preetha Kumar) | Y | Y | Y | Y | N | N | Y |
| Local Counter Fraud representatives (Martyn Tait) | Y | Y | Y | Y | N | N | Y |
| External Audit representatives (Campbell Dearden, Mark Kirkham) | Y | Y | Y | Y | Y | Y | Y |
| Governor representatives (Jamie Rickleton / Anne Carlile***) |
N | Y*** | Y*** | Y*** | Y*** | N | N |
Internal Audit and Counter Fraud services was provided by Audit One. ternal audit services was provided to the audit team from Mazars Plc.
In addition to the officers that regularly attend the committee, invitations were extended to members of the Executive Team and senior managers who attended meetings to present papers and provided assurances as required.
Reports made to the Board of Directors
The Chair of the Audit Committee makes an assurance, escalation and advisory report regarding the most recent meeting of the committee to the ne t available Board of Directors meeting. This report seeks to assure the Board on the main items discussed by the Committee, and should it be necessary, to escalate to the Board any matters of concern or urgent business. The Board may then decide to give direction to the Committee as to how the matter should be taken forward or it may agree that the Board deals with the matter itself.
The below table outlines the dates that the assurance and escalation reports were presented by the Chair of the Audit Committee to the Board of Directors meetings
| Date of Meeting | Assurance and escalation report to Board by Chair of the Audit Committee |
|---|---|
| 8th May 2024 | 5th June 2024 |
| 7th August 2024 | 4th September 2024 |
| 6th November 2024 | 4th December 2024 |
| 2nd February 2025 | 30 April 2025 |
In addition to the reports made by the Chair of the Committee this Audit Committee annual report is also included in the Trust Annual Report and Accounts for completeness, which is submitted to the Board of Directors in June.
The work of the Committee during 2024/25
For 2024/25 the Chair and members of the Audit Committee confirm that the committee has fulfilled its role as the primary governance and assurance committee in accordance with its Terms of Reference.
In 2024/25 the committee approved the work plans for both the internal and e ternal auditors and the counter fraud service. It received and reviewed both regular progress reports and concluding annual reports for the work of internal and e ternal audit and the counter fraud team. This allowed the committee to determine its level of assurance in respect of progress with various pieces of work and the findings. These reports have also provided assurance on the Trust’s internal controls. The committee assessed the effectiveness of these functions by reviewing the periodic reports from the auditors and monitoring the pre agreed key performance indicators.
Programme of Works
• Reviewed the Patient Incident Reporting Framework (PSIRF) which sets out how Trusts review and learn from incidents and events which occur including both negative and positive incidents/events. The PSIRF plan and policy were signed off by the Board and ICB during November 2023 and the implementation of PSIRF commenced across the organisation on 22 January 2024, and since then significant engagement has been undertaken both internally and externally. The Committee requested six monthly updates for assurance that the Trust is adhering to the new framework and to ensure the Trust is learning from incidents which is fundamentally a new way reviewing incidents. Patient Safety Incident Investigations (PSII) are now scheduled to the Audit Committee cycle to ensure learning and improvement in patient safety.
•Reviewed Emergency Preparedness, Resilience and Response ( PRR) including Staff Attack Alarms with assurance provided the Trust compliance with PRR code standards and staff attack personal alarms with plans in place to address non compliance actions by the end of Quarter 2. A standardised checklist has been introduced across all inpatient wards for the tracking assets and upgrading of equipment across all sites.
• Violence and aggression incidents across the organisation continue to be closely monitored, and a specific violence and Aggression Group has been established to focus on what can be put in place to provide a safer environment for staff and patients.
•Reviewed the arrangements of cyber security and risks against the national strategy on cyber which sets out a vision to reduce cyber security risks across health and social care which feed into the organisations approach to cyber security and will be measured via the Data Security and Protection Toolkit providing assurance at annual checks to ensure the Trust are meeting the standards.
• Reviewed the process for records management transferring paper records digitally with the Trust developing a destruction policy due implemented in September 2024 to enable the life cycle of a record to continue in line with the Records Management Code of Practice.
• Reviewed and challenged the rostering and overview process with the 3 year roll out of the Allocate system which NTW Solutions part of the programme to have a consistent group approach.
• Assessed the integrity of the Group’s consolidated and NTW Solutions standalone financial statements for the year ended 31 March 2025.
• Reviewed the Annual Governance Statement in light of the Head of Internal Audit opinion, the ternal Audit opinion relating to the year end and any reports issued by CQC and NHS England.
• Reviewed ternal Audit’s findings and opinions on the Quality Report, the securing of economy, efficiency and effectiveness, and the areas of Annual Report subject to audit review.
• Considered whether the Trust’s Board Assurance Framework (‘BAF’) and Corporate Risk Register were complete, monitored, fit for purpose and in line with Department of Health expectations, as well as receiving assurance on the ongoing process for review.
• Reviewed the arrangements by which staff may raise in confidence concerns about possible improprieties in matters of financial reporting and control, clinical equality, patient safety or other matters.
• Reviewed the process established by the Trust to ensure compliance with NHS Foundation Trust Code of Governance.
• Challenged and approved the Internal Audit programme, Local Counter Fraud Service annual plans and detailed programmes of work for the year. The Audit Committee confirmed the effectiveness of Internal Audit and Counter Fraud and the adequacy of their staffing and resources.
• Considered the major findings of Internal Audit and Counter Fraud throughout the year. The Audit Committee agreed that the remedial actions proposed were appropriate and then monitored the timely implementation of those remedial actions by management.
• Reviewed the work of other Board Committees and considered how matters discussed at those committees impacted the work of the Audit Committee.
Board Assurance Frame work
The Audit Committee has a responsibility to ensure that the Trust’s system of risk management is adequate in both identifying risks and how those risks are managed. The Trust’s principal risks, and the mitigating controls are reflected in the Board Assurance Framework (‘BAF’) and Corporate Risk Register (‘CRR’). During 2023/24, the Audit Committee contributed to the formal annual review of the BAF and CRR.
A significant piece of work was undertaken with Board colleagues in September 2023, to review the Trust Risk Appetite and Board Assurance Framework following the new Trust Strategy ‘With you in mind’, new strategic ambitions, challenges and planning priorities for the year and to reflect working within a system which the previous BAF did not cover. The new BAF and Risk Appetite was approved by the Board November 2023. Audit Committee approved the Risk Management Policy on 10 January 2024. Since that time, and during the past 12 months, there has been a significant amount of work to embed the new Risk Management Policy and framework across the organisation, to ensure robust processes are in place to ensure the identification, management, and escalation of risk from ward to Board.
The Audit Committee provided challenge and scrutiny as to the system for the regular assessment and review of the principal risks and mitigating controls reflected in the BAF. This includes a cycle of attendance from Board Committee Chairs to report to the Audit Committee on their approach to the management of risks aligned to the respective committees. The Audit Committee reviews the BAF in its entirety at each meeting and provides assurance to the Board that risks are being managed effectively, where risks need to be reviewed, escalated or de escalated and assurance that the BAF continues to be reflected in the priority areas of Internal Audit planning for the Trust.
Given the significant work undertaken since January 2024 around the implementation and embedding of the new risk management policy and process, a specific request was made to undertaken two separate audits of the BAF and risk management (usually undertaken as a single audit). This was to ensure robust testing of the new processes in place.
Internal Audit of both the BAF and Risk Management processes received a ‘substantial’ level of assurance. The BAF identified no actions or recommendations, and the risk management report identified two recommendations (low risk), which were complete at the time of the report being issued.
Finally, the Audit Committee reviewed the Head of Internal Audit Opinion, presented to the Audit Committee on 8 May 2024. The Trust was provided with good assurance on the basis that there is “sound system of internal control, governance and risk management designed to meet the organisations objectives and that controls are generally being applied consistently”. The Head of Internal Audit Opinion for the 2024/25 year will be reviewed at the Audit Committee scheduled to take place in May (as draft) and June (final).
Annual Governance Statement
The Audit Committee is required to consider the Annual Governance Statement and determine whether it is consistent with the Audit Committee’s view on the Trust’s system of internal control.
During the year, matters have been brought to the attention of the Audit Committee, mainly through the reports of Internal Audit. Therefore, the Audit Committee needed to formally consider these matters in forming its conclusion on the Annual Governance Statement for 2023/24. This was supported by other Audit Committee reviews such as of the Board Assurance Framework, Corporate Risk Register, Head of Internal Audit Opinion and CQC registration.
After due challenge and debate, the Audit Committee concluded that the matters identified together with the remedial actions taken meant that its view on the Trust’s system of internal control was consistent with the Annual Governance Statement. Accordingly, the Audit Committee supported the Board’s approval of the Annual Governance Statement for 2023/24. The Annual Governance Statement for the 2024/25 year will be submitted to the June 2025 meeting of the Audit Committee, prior to inclusion in the 2024/25 Trust Annual Report and Accounts.
Clinical Audit
Clinical Audit continued to be reported to the Quality and Performance committee of the Board (‘Q&P’) and not to the Audit Committee. One member of the Audit Committee is also a member of Q&P. Therefore, the Audit Committee is able to monitor any issues raised by Clinical Audit to Q&P.
In addition, the Chair of Q&P attends a minimum of one meeting of the Audit Committee per year to bring to the attention of the Audit Committee any matters raised by Clinical Audit alongside an assurance update on the management of risks aligned to the Q&P Committee. This ensures that the Audit Committee is aware of any key issues raised by Clinical Audit but does not add unnecessary bureaucracy, duplication or contradiction into the process.
External Audit
The Audit Committee places great importance on ensuring that there are high standards of quality and effectiveness in the Trust’s e ternal audit process. Mazars was required to report to the Trust whether:
• The financial statements for the 2023/24 year were prepared in accordance with directions under Paragraph 25 of Schedule 7 of the National Health Service Act 2006.
• The financial statements for 2023/24 complied with the requirements of all other provisions contained in, or having effect under, any enactment which is applicable to the financial statements.
• The Trust has made proper arrangements for securing economy, efficiency and effectiveness.
Following the Council of Governors meeting on 9th November 2023, the Governors, led and supported by the Audit Committee embarked on a tender exercise for appointment of an e ternal auditor whose contact was due to end 31 May 2024. The e ternal audit exercise covered the provision of e ternal audit services, covering audit of the Trusts financial statements, the annual accounts for the Charity along with NTW Solutions accounts. Only a single bid was received by the closing date, which was from Mazars, the Trusts current e ternal audit provider. The panel agreed that the bid was a very high standard and offered all the assurance the Trust require.
The Council of Governors, on 21 March 2024, ratified the decision to award the External Audit contract to Mazars to commence 1 June 2024, for an initial period of 36 months with an option to extend for a further 24 months as Mazars are providing the Trust with a good level of services, performing well in the work that they undertake.
The Trust has a policy in place for non audit services provided by ternal Audit, which has been approved by the Council of Governors.
On 8 May 2024, Mazars presented the audit plans for the Trust (and Group) to the Audit Committee. The audit plan was challenged robustly, particularly in terms of timing, resources required versus fee proposed, impact on the Trust’s day to day activities, areas of audit risk, interaction with Internal Audit and the quality and independence of the Mazars team.
Following the challenge and debate, the Audit Committee was satisfied that the audit plan for 2023/24 was appropriate for achieving the goals of the audit and that the proposed fee was reasonable for the audit of an entity of the size and complexity of the Trust.
Throughout the audit process, Mazars reported to the Audit Committee, noting any issues of principle or timing identified by the audit, changes in the ternal Auditor’s assessment of risk and any significant control weaknesses or errors identified.
Mazars identified no changes in their assessment of risk, nor did they identify any significant control weaknesses. The audit did identify some instances of misstatement. None of the unadjusted misstatements identified were assessed as material. The Trust’s financial statements 2023/24 were adjusted for all the matters identified.
During 2024/25 Mazars also undertook the audit of NTW Solutions Limited and an independent examination of the Trusts Charitable Funds, Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust Charity.
The outcome of the External Audit on the Trust (and Group) accounts for the 2024/25 year will be presented to the Audit Committee at the June 2025 meeting ahead of presentation to the Board of Directors.
The Audit Committee considered the scope of the work being requested from Mazars and the proposed fee. The Audit Committee also confirmed that the scope of the work had been subject to Mazars’ own internal independence review. After careful consideration, the Audit Committee agreed that the proposed scope of work and associated fee would not impair the independence of the External Auditor.
Internal Audit and Counter Fraud
The Trust has an established Internal Audit and Counter Fraud function, provided by AuditOne (hosted by CNTW), to provide independent objective assurance and advisory oversight of the operations and systems of internal control within the Trust. AuditOne is an NHS audit consortium providing services to a number of NHS trusts in northern England.
AuditOne helps the Trust to accomplish its objectives by bringing a systematic, disciplined approach to evaluate and improve the effectiveness of risk management, control and governance processes.
The committee reviewed, challenged and approved the proposed AuditOne audit and counter fraud plans and budgets for 2024/25. The Audit Committee have had continual oversight of any remedial actions required were undertaken according to the agreed timescales.
Policies
The committee has delegated responsibility for the review and oversight of the Declarations of Interest and Fraud Bribery and Corruption policies.
The Declaration of Interest Policy was reviewed and updated during 2024/25 to include further clarity in relation to indirect interests, in particular, relationships and Bribery and Corruption. The Declaration of interest Policy is reviewed on an annual basis as part of the Committee regular cycle of business.
In relation to the Raising Concerns (whistleblowing) policy, the application of that policy is managed by the Quality and Performance Committee and People Committee. Any significant matters arising are brought to the attention of the Audit Committee by the Chair of both mentioned Committees. However, the Audit Committee is responsible for assessing the independence, autonomy and effectiveness of the resolution of any significant matters subject to a whistleblowing event. No such matters were brought to the attention of the Audit Committee during the year.
Following key changes to the Fit and Proper Persons Test which came into effect for all NHS Trusts from 30 September 2023, a Fit and Proper Persons Test policy has been devised, reviewed and approved on 31 January 2024 Audit Committee and Board of Directors meeting 6 March 2024. The outcome of the Fit and Proper Test annual review for the 2024/25 year will be presented to the June meeting of the Audit Committee and July meeting of the Board of Directors.
Annual Review of Audit Committee Effectiveness
Audit Committee members carried out a self assessment exercise during March 2025 in line with the requirements and guidance of the newly published NHS Audit Committee Handbook March 2024. The feedback was very positive in the majority of areas which cover composition, establishment and duties; compliance with legislation and regulation; internal control and risk management; Internal Audit, Counter Fraud; clinical audit; and annual accounts and disclosure statements.
Summary
The above outlines the work of the Audit Committee during the past year upon which the assurances given to the Board of Directors during the year have been based.
The Committee recognises the challenges which the Trust has faced by the Trust and the wider health and care system in terms of the challenges relating to financial planning, service delivery, workforce planning, increasing demands, changes to legislation and governance structures associated with the establishment of Integrated Care Boards and ‘placed based’ working.
As the primary governance committee to the Board of Directors the Audit Committee presented its independence from operational management by not having executive membership, although executive directors support the committee by providing information and content only.
It added value by maintaining an open and professional relationship with internal and e ternal audit and counter fraud. It carried out its work diligently discussing issues openly and robustly and kept the Board of Directors appraised of any possible concerns or risks. The Audit Committee fulfilled its programme of work for 2024/25 and provided assurances to the Board for any issues referred to it. It took assurances from the Internal and External Audit teams on key matters.
The Chair of the Audit Committee considers that the committee has fulfilled its role as the Board of Directors senior governance committee and provided assurance to the Board on adequacy and effective operation of the organisation’s internal control systems. The Committee is confident that key controls will be maintained through the Trust’s governance framework in order to assist the Trust in achieving its objectives.
Members of the Audit Committee would like to thank all those who have responded to its requests during the year and who have supported it in carrying out its duties.
The Board of Directors ensure that they develop an understanding of the views of the Governors and members about the Foundation Trust by:
• Board members attending all meetings of the Council of Governors, and sub-groups.
• Council of Governors’ attendance at meetings of the Board of Directors.
• Annual joint meeting of the Council of Governors and Board of Directors.
• Informal opportunities to network.
• Governor Representatives attending sub-committees of the Board, provides a further opportunity to share views.
The Council of Governors has been established to include both elected and appointed Governors and their roles and responsibilities are set out in the Trust’s Constitution. Elected Governors consist of public Governors, service user and carer Governors and staff Governors, and appointed Governors are from partner organisations. The composition of the Council of Governors is also detailed in the Trust’s Constitution available on the website.
Service users and carers are represented separately with seven seats each, reflecting our commitment to these groups. Public Governors represent those in their local authority area resulting in the Trust having seven public Governors, one for each local authority area within the Trust footprint. Any individual who lives outside one of the seven local government areas but within England and Wales may become a public member and they will be represented by the Newcastle upon Tyne/Rest of England and Wales constituency.
Substantively employed staff are automatically members unless they decide to opt out, which was determined by the Trust in partnership with Staff Side. They are represented by one governor for medical staff and three each from non-clinical and clinical areas.
We have also sought to ensure that our partners including local authorities, universities, and voluntary organisations, are represented.
The tenure for elected and appointed Governors comes to an end after three years, but they may seek re-election by the members of their constituency for a maximum of a further two terms of office of up to three years each. An elected Governor may not hold office for longer than a continuous period of nine consecutive years.
Governor Elections 2024/2025
Governor Elections took place in November 2024 for the following constituencies:
| Constituency | No. of seats | No. of candidates | Total number of valid votes | Elected No. of votes |
|---|---|---|---|---|
| Service User: Adult Services | 1 | 3 | 24 | 9 |
| Carer: Adult Services | 2 | 3 | 27 | 13 |
| Carer: Neuro-Disability Services | 1 | 1 | 8 | 6 |
| Public: Cumbria (North) | 1 | 2 | 29 | 20 |
| Staff: Non-Clinical | 1 | 1 | 429 | 231 |
| Staff: Clinical | 1 | 6 | 259 | 81 |
| Staff: Medical | 1 | 2 | 78 | 63 |
The following seats were elected unopposed.
| Constituency | No. of seats | No. of candidates |
|---|---|---|
| Service User: Learning Disability Services | 1 | 1* |
| Public: South Tyneside | 1 | 1 |
| Public: Newcastle, Rest of England & Wales | 1 | 1 |
| Public: Northumberland | 1 | 1** |
* Service User: Learning Disabilities
Following the elections candidate elected withdrew from the Council December 2024.
**Public: Northumberland
Following the elections candidate elected withdrew from the Council December 2024.
The following seats remained vacant as of 28 November 2024.
| Constituency | No. of seats |
|---|---|
| Service User: Older Peoples Services | 1 |
| Service User: Children and Young Peoples Services | 1 |
| Public: North Tyneside | 1 |
| Local Authority: Gateshead Council | 1 |
Following the Governor Election process undertaken in November 2024, six seats within the Council remained vacant. Following the recommendation and approval from the Council of Governors in March 2023 the Trust adopted appointing non-voting Shadow Governors bringing members onto the Council in a Shadowing Capacity this will help to fill vacant seats of the Council until the next election in October 2025.
The benefits of proceeding with the shadow governor process were to ensure that the Council of Governors are fully represented while the Trust continue its journey to address the challenges faced by the Trust and wider health and care system without the additional cost of holding a bi-election. As of 31 March 2025, the Council of Governors gained one Shadow Governor for Public Northumberland constituency. Below are the current vacant seats with the Council until the next elections in October 2025.
| Constituency | No. of seats |
|---|---|
| Service User: Learning Disability Services | 1 |
| Service User: Older Peoples Services | 1 |
| Service User: Children and Young Peoples Services | 1 |
| Service User: Adult Services | 1 |
| Public: North Tyneside | 1 |
| Local Authority: Gateshead Council | 1 |
Table 13: Membership of the Council of Governors and Attendance at Council of Governor General meetings 1 April 2024 – 31 March 2025
| Governor | Constituency | Start date | Stood down date | Current term | Attendance/total number of meetings held |
|---|---|---|---|---|---|
| Elected Governors (service users, carers and public) | |||||
| Fiona Grant | Service User, Adult Services | 01.12.14 | 31.11.25 | 3rd | 1/1 |
| *Tom Rebair | Service User, Adult Services | 01.03.21 | - | 2nd | 2/3 |
| Anita Kniveton | Service User, Adult Services | 01.12.24 | - | 1st | - |
| Russell Stronach | Service User, Autism Services | 01.01.22 | - | 2nd | 2/3 |
| ***Russell Bowman | Service User, Neuro Disability Services | 01.01.23 | - | 3rd | 3/3 |
| Anne Carlile | Carer, Adult Services | 01.04.16 | 31.11.25 | 3rd | 2/2 |
| Jane Noble | Carer, Adult Services | 01.03.22 | 31.11.25 | 3rd | 0/3 |
| Fiona Regan | Carer, Learning Disability and Autism | 01.12.18 | - | 3rd | 1/3 |
| Roy Fussey | Carer, Adult Services | 01.12.24 | - | 1st | - |
| Shannon Fairhurst | Carer, Children and Young Peoples Services | 01.12.23 | - | 1st | 2/3 |
| Rosie Lawrence | Carer, Learning Disability Services | 01.12.23 | - | 1st | 0/3 |
| Jessica Juchau-Scott | Carer, Older People’s Services | 01.01.23 | - | 2nd | 2/3 |
| Neil Newman | Carer Governor, Neuro-Disability Services | 18.03.23 | - | 1st | 3/3 |
| Mary Laver | Public Governor, North Tyneside | 01.01.23 | 31.11.24 | 2nd | 1/3 |
| Mahdi Hassan | Public, Newcastle/Rest of England and Wales | 01.12.24 | - | 1st | - |
| Jamie Rickelton | Public, Gateshead | 01.01.23 | - | 2nd | 0/3 |
| Heather Lee | Public, South Tyneside | 01.12.24 | - | 1st | 2/3 |
| Jodine Milne-Reader | Public, Sunderland | 01.01.23 | - | 2nd | 2/3 |
| Tom McLaughlan | Public, Cumbria | 01.12.24 | - | 1st | - |
| **Serena Ayres | Public, Northumberland | 01.02.24 | - | 1st | - |
| Staff Governors | |||||
|---|---|---|---|---|---|
| Daniel Cain | Staff, Non-Clinical | 01.01.22 | 31.11.25 | 2nd | 1/1 |
| Gemma Miles | Staff, Non-Clinical | 01.12.24 | 1st | - | |
| Dr Thomas Lewis | Staff, Medical | 01.01.22 | - | 2nd | 2/3 |
| Claire Keys | Staff, Clinical | 01.12.15 | 31.11.25 | 3rd | 3/5 |
| Adrian Amin | Staff, Clinical | 01.12.25 | 1st | 3/3 | |
| Emma Silver Price | Staff, Non-Clinical | 01.12.22 | - | 2nd | |
| Doreen Chananda | Staff, Clinical | 01.01.22 | - | 2nd | |
| Amber Cormack | Staff, Clinical | 01.12.23 | - | 1st | |
| Adrian Anim | Staff, Clinical | 01.12.24 | - | 1st | |
| Siobhan Watson | Staff, Non-Clinical | 01.12.23 | - | 1st |
| Appointed Governors | |||||
|---|---|---|---|---|---|
| Cllr Kelly Chequer | Local Authority, Sunderland | 08.08.19 | - | 4th | 2/3 |
| Cllr Ruth Berkely | Local Authority, South Tyneside | 01.07.23 | - | 1st | 3/3 |
| Cllr Jane Shaw | Local Authority, North Tyneside | 01.07.23 | - | 1st | 2/3 |
| Cllr Maria Hall | Local Authority, Gateshead | 01.06.19 | 10.05.24 | 4th | - |
| Cllr Wendy Pattison | Local Authority, Northumberland | 01.05.22 | - | 2nd | 1/3 |
| Cllr Miriam Mafemba | Local Authority, Newcastle | 01.05.23 | - | 2nd | 1/3 |
| Prof Sithandazile Masuku | Northumbria University | 01.12.23 | - | 1st | 0/3 |
| Andrew Kingston | Newcastle University | 01.12.24 | - | 1st | - |
| Yitka Graham | Sunderland University | 01.01.23 | 2nd | 0/3 | |
| Joy Duxbury | Cumbria University | 01.03.25 | 1st | - | |
| Bea Groves McDaniel | Difference North East | 01.12.23 | 1st | 1/3 | |
| Julia Clifford | iCan Health and Fitness CIC | 01.06.23 | 1st | 3/3 |
There have been four formal meetings of the Council of Governors during 2024/25, including the Annual Members’ Meeting. There has also been a number of development sessions as determined by the Governors’ Steering Group. It is a fundamental principle of the Health and Care Act 2022 that no governor shall receive any form of salary, but reasonable reimbursement will be made for allowable e penses. The Trust’s policy is that reasonable expenses will be reimbursed to attend authorised training and induction events, and meetings attended relating to their role as a Governor.
*Lead Governor
** Shadow Governor
****Re-joined constituency replacing a Governor stood down
Table 14: Attendance of Board members at formal Council of Governors’ meetings (including Annual Members’ Meeting/AG ).
| Council of Governors’ General meetings attended b Board members April 2024 – March 2025 | |
|---|---|
| Board Member | Attendance/total number of meetings held |
| Darren Best, Chair | 3/3 |
| David Arthur, Non-Executive Director / SID | 2/3 |
| Paula Breen, Non-Executive Director | 1/3 |
| Michael Robinson, Non-Executive Director | 3/3 |
| Brenda Hill, Non-Executive Director | 3/3 |
| Louise Nelson, Non-Executive Director | 1/3 |
| Robin Earl, Non-Executive Director | 1/2 |
| Vikas Kumar, Non-Executive Director | 2/3 |
| Rachael Bourne, Non-Executive Director | 3/3 |
| James Duncan, Chief Executive (from 1/2/22) | 3/3 |
| Dr Rajesh Nadkarni, Deputy Chief Executive/Medical Director | 1/3 |
| Ramona Duguid, Chief Operating Officer | 2/3 |
| Lynne Shaw, Director of Workforce and Organisational Development | 3/3 |
| Kevin Scollay, Executive Finance Director | 2/3 |
| Sarah Rushbrooke, Executive Director Nursing, Therapies and Quality Assurance | 1/3 |
Engagement with the public, members and partner organisations and their views relating to the forward plan
The Board has regard to the views of the Council of Governors in preparing the Trust’s Operational Plans and Strategic Plans. The Council of Governors is consulted on the development of forward plans and any significant changes for the delivery of the Trust’s Operational Plan. In 2024/25 the Council of Governors as well as service users, carers and members of the public were fully involved in the development of the of the Trust’s Quality Priorities for 2024/25.
Membership
Our approach to membership is one of inclusivity, with membership available to everyone who:
• Is at least 14 years old.
• Lives in the areas served by the Trust i.e. Cumbria, Northumberland, North Tyneside, South Tyneside, Gateshead, Sunderland and Newcastle, or the rest of England and Wales.
• Has used our services in the last six years, or
• Has cared for someone who has used our services in the last six years.
• Is a member of staff on a permanent contract or who has worked for the Trust for 12 months or more.
As of 31 March 2025, the Trust reported a membership of 11,530 public, service users and carers and 8,633 staff (see the table below for details of numbers per constituency).
Our Trust has considerable engagement via e-bulletins, the Trust website and social media channels and the provision of advice, support and guidance to our members and the public as a whole during what has been a challenging year for everyone.
The Governors’ Steering Group has delegated responsibility for monitoring the Membership Engagement and Governor Development Plan. The plan has been refreshed during the year, acknowledging the need to consider alternative and more innovative ways of engaging with members, the public and other stakeholders.
The Trust membership remains relatively static with ongoing work in targeted recruitment during 2024/25 particularly within hard-to-reach groups. Although the Trust continues to work hard to build, develop and maintain the membership base to ensure appropriate community representation, it is the view of the Trust and the Council of Governors, that following the change in Governor duties as part of the Health and Social Act 2012 implementation, to represent the public as a whole, our focus will continue to be on ‘ quality’ of our engagement and communication.
Our target is to maintain a focus of activity based on ensuring the membership is refreshed and that membership figures are maintained. Whilst acknowledging the work to increase user and carer membership it is important that we introduce a more targeted approach to communication and engagement to ensure dialogue with members and the public is more meaningful and aligned to specific areas of service change and development. This includes ensuring good representation within the different localities we serve and engaging in new and more meaningful ways with the community as a whole.
Members are free to contact Governors and/or Directors at any time via the Corporate Affairs Team (telephone number 0191 245 6827) or email corporateaffairs
Table 15: Analysis of membership as of 31 March 2025
| Constituency | 31 March 2023 | 31 March 2024 | 31 March 2025 |
|---|---|---|---|
| Public | |||
| Cumbria | 86 | 85 | 89 |
| Gateshead | 926 | 927 | 921 |
| Newcastle upon Tyne/Rest of England and Wales | 3,394 | 3,435 | 3,432 |
| Northumberland | 1,283 | 1,263 | 1,259 |
| North Tyneside | 1,400 | 1,403 | 1,399 |
| South Tyneside | 780 | 780 | 778 |
| Sunderland | 1,965 | 1,938 | 1,934 |
| Out of Trust Area | 35 | 36 | 44 |
| Sub total | 9,869 | 9,867 | 9856 |
| Service Users | |||
|---|---|---|---|
| Adults | 367 | 350 | 152 |
| Children and young people | 135 | 133 | 505 |
| Learning disability | 87 | 81 | 101 |
| Neuro-disability | 110 | 107 | 81 |
| Older people | 36 | 34 | 79 |
| Unknown* | 53 | 53 | 54 |
| Sub total | 788 | 758 | 972 |
| Carers | |||
|---|---|---|---|
| Adults | 145 | 151 | 351 |
| Children and young people | 515 | 506 | 133 |
| Learning disability | 102 | 101 | 78 |
| Neuro-disability | 79 | 76 | 106 |
| Older people | 80 | 79 | 34 |
| Sub total | 921 | 913 | 702 |
| TOTAL | 11,578 | 11,538 | 11,530 |
| Staff | |||
|---|---|---|---|
| Unspecified | 68 | 70 | 66 |
| Medical | 480 | 571 | 497 |
| Other Clinical | 3,445 | 3,562 | 3,459 |
| Non Clinical | 4,571 | 4,959 | 4,611 |
| Total All Staff | 8,564 | 9,162 | 8,633 |
| TOTAL MEMBERS | 20,142 | 20,700 | 20,163 |
*The total number of unknowing relates to both Service User and Carer constituencies.
Declaration of Interests
Along with Board members, all Governors are asked to declare any interest on the Register of Governors’ Interests at the time of appointment and annually every March. The register is available for inspection on the internet at www.cntw.nhs.uk or on request, from Kirsty Allan, Corporate Governance Manager, Chief Executive’s Office, St. Nicholas Hospital, Jubilee Road, Gosforth, Newcastle upon Tyne, NE3 3XT. (corporate.
All Governors on the Council of Governors have, on appointment, confirmed that they meet the Fit and Proper Persons Test and complete an annual declaration confirming that they continue to be a fit and proper person.
NHS Foundation Trust Code of Governance
Cumbria. Northumberland, Tyne and Wear NHS Foundation Trust has applied the principles of the NHS Foundation Trust Code of Governance on a ‘comply or e plain’ basis. The NHS Foundation Trust Code of Governance, most recently revised and published April 2023, is based on the principles of the UK Corporate Governance Code.
The Board of Directors is collectively responsible for the exercise of the powers and the performance of the Trust. As a unitary Board all directors have joint responsibility for every decision of the Board of Directors and share the same liability. This does not impact upon the responsibilities of the Chief Executive as the accounting officer.
The Board has a Scheme of Reservation and Delegation and Standing Financial Instructions, and delegates as appropriate to committees or senior management, e.g., the delegation to officers to certify payments up to pre-determined levels. However, the Board remains responsible for all of its functions, including those delegated.
The general duty of the Board and of each director individually, is to act with a view to promoting the success of the organisation so as to maximise the benefits for the members of the Trust as a whole and for the public. Its role is to provide leadership of the Trust within a framework of prudent and effective controls, which enables risk to be assessed and managed. It is responsible for:
• Ensuring the quality and safety of healthcare services, education, training, and research delivered by the Trust and applying the principles and standards of clinical governance set out by the Department of Health, NHS England, the Care Quality Commission, and other relevant NHS bodies.
• Setting the Trust’s vision, values and standards of conduct and ensuring that its obligations to its members are understood clearly communicated and met. In developing and articulating a clear vision for the Trust, it should be a formally agreed statement of the Trust’s purpose and intended outcomes which can be used as a basis for the Trust’s overall strategy, planning and other decisions.
• Ensuring compliance by the Trust with its licence, its constitution, mandatory guidance issued by NHS Improvement, relevant statutory requirements, and contractual obligations.
• Setting the Trust’s strategic aims at least annually, taking into consideration the views of the Council of Governors, ensuring that the necessary financial and human resources are in place for the Trust to meet its priorities and objectives and then periodically reviewing progress and management performance.
• Ensuring that the Trust exercises its functions effectively, efficiently, and economically.
• The general duty of the board of directors, and of each director individually, is to act with a view to promoting the success of the corporation to maximise the benefits for the members of the corporation as a whole and for the public.
The general duties of the Council of Governors are:
• To hold the Non-Executive Directors (NEDs) individually and collectively to account for the performance of the Board of Directors, which includes ensuring the Board of Directors acts so that the Trust does not breach the terms of its licence; and
• To represent the interests of the members of the NHS Foundation Trust as a whole and the interests of the public.
In addition, the statutory roles and responsibilities of the Council of Governors are to:
• Appoint and, if appropriate, remove the Chair.
• Appoint and, if appropriate, remove the other NEDs.
• Decide the remuneration and allowances, and other terms and conditions of office, of the Chair and the other NEDs.
• Approve (or not) any new appointment of a Chief Executive.
• Appoint and, if appropriate, remove the Trust’s auditor.
• Receive the Trust’s annual accounts, and the annual report at a general meeting of the Council of Governors.
• Provide views to the Board when the Board is preparing the document containing information about the Trust’s forward planning, noting that the Board must have regard to the views of the Council of Governors.
• Approve significant transactions.
• Approve an application by the Trust to enter into a merger, acquisition, separation or dissolution.
• Decide whether the Trust’s non-NHS work would significantly interfere with its principal purpose, which is to provide goods and services in England.
• Approve amendments to the Trust’s constitution.
• Require, if necessary, one or more directors to attend a Council of Governors meeting to obtain information about performance of the Trust’s functions or the directors' performance of their duties, and to help the Council of Governors to decide whether to propose a vote on the Trust’s or directors’ performance.
The Council of Governors is not responsible for the day to day running of the organisation and cannot therefore veto decisions made by the Board.
The Council of Governors has established a Nominations Committee in-line with the requirement within the Trust’s Constitution, and its Terms of Reference are included on the Trust website. Its role includes making recommendations to the full Council of Governors on the appointment of the Chair and Non-Executive Directors (NEDs) and the associated remuneration and allowances and other terms and conditions.
In addition to the core membership, the Senior Independent Director will be invited to attend and co-chair any discussion in respect of its duties pertaining to the performance of, and/or appointment/reappointment of the Chair.
During the year, the Nominations Committee met twice. Attendance requirements varied based on the business discussed. Membership and attendance at the Nominations Committee is shown in table 16 below:
Table 16: Nominations Committee Membership and Attendance
| Name | Attendance/total number of meetings held |
|---|---|
| Darren Best, Co-Chair | 2/2 |
| Anne Carlile, Lead Governor/Carer Governor Adult Services* (until November 2024) | 1/1 |
| Tom Rebair, Deputy Lead Governor/Service User Governor Adult Services* | 2/2 |
| Fiona Grant, Service User Governor for Adult Services (until November 2024) | 1/1 |
| Yitka Graham, Appointed Governor Sunderland University (from September 2023) | 0/2 |
| Emma Silver-Price, Non-clinical Staff Governor (from January 2024) | 2/2 |
| Sithandazile Masuku, Appointed Governor, Northumbria University (from January 2024) | 1/2 |
| Debbie Henderson, Director of Communications and Corporate Affairs | 2/2 |
| David Arthur, Senior Independent Director (in attendance) (until January 2025) | 0/1 |
* Co-Chairs of the Governors’ Nomination Committee
The Nominations Committee is jointly chaired by the Trust Chair and Lead Governor.
The work undertaken by the Nominations Committee entails reviewing job descriptions and person specifications, receiving an update on Chair and Non-Executive Director performance based on annual appraisal processes, agreeing processes for re-appointment and appointment of the Chairman and other NEDs, considering the need for external support, and the associated work underpinning such processes. In addition, the Committee performs a regular review of the Chair’s and other N Ds’ performance and their remuneration in line with national guidance and recommendations. The Nomination Committee also review the overall skill mix of the Board when considering appointment/reappointments of the Chair and NEDs.
The Nominations Committee’s also includes overseeing the process relating to the termination, where this is not because of resignation, of the Chair or another NED coming to the end of their term. This role applies in limited circumstances such as gross misconduct or a request from the Board of Directors for the removal of a particular NED.
In delivering its remit, the Committee undertook the following:
• Received the performance development reviews for the Non-Executive Directors and Chair.
• Reviewed the proposal to re-appoint Louise Nelson and Brendan Hill, Non-Executive Directors for a second term of office to commence 1 October 2024 – 30 September 2027 and Brendan Hill to continue as Vice Chair during the period which was fully supported by the Council of Governors at its meeting on 19 September 2024.
• Reviewed and approved the recommendation to extend Michael Robinson, Non-Executive Director’s second term of office to 30 September 2025 and appoint Michael Robinson as Senior Independent Director during this period.
• In preparation for the departure of Paula Breen, Non-Executive Director on 31 March 2025, the Committee discussed and agreed to undertake a recruitment process outlining both Non-Executive Director roles to chair the Mental health Legislation Committee and Resource, Business Assurance Committee with a possible third Non-Executive Director to be recruited for Digital. This process will be undertaken in quarter1 and 2 of 2025/26.
The Committee continues to review the appointment/re-appointment process and timeline for current Non-Executive Directors to ensure appropriate succession planning is in place. A review of the terms, conditions and remuneration of the Chair and Non-Executive Directors will be undertaken in 2025/26.
NHS England is the Independent Regulator for NHS Foundation Trusts. They have published an NHS Foundation Trust Code of Governance which brings together the best practice of public and private sector corporate governance.
The Trust has applied the principles of the NHS Foundation Trust Code of Governance on a comply or explain basis. The NHS Foundation Trust Code of Governance, most recently revised and published in April 2023, is based on the principles of the UK Corporate Governance Code. The Trust remains compliant with all provisions of the code. The Board of Directors, received a full assurance report on:
• Individual requirements of the Code.
• Confirmation of compliance (or an explanation of non-compliance where required).
• Evidence of compliance.
• Clarification on reporting and disclosure requirements.
All requirements where supporting information is required to be made available is available either on request or on the Trusts website.
The Trust continues to keep governance arrangements under review to ensure their effectiveness and no material governance concerns were identified.
All requirements where supporting information is required to be made available is available either on request or on the Trusts website.
Compliance with the NHS Code of Governance
| Table 17 | NHS Code of Governance Compliance | ||
|---|---|---|---|
| Provision | Requirement | Trust Position | Evidence |
| Section A 2.1 | The board of directors should assess the basis on which the Trust ensures its effectiveness, efficiency, and economy, as well as the quality of its healthcare delivery over the long-term, and contribution to the objectives of the ICP and ICB, and place-based partnerships. The board of directors should ensure the Trust actively addresses opportunities to work with other providers to tackle shared challenges through entering partnership arrangements such as Provider Collaboratives. The Trust should describe in its annual report how opportunities and risks to future sustainability have been considered and addressed, and how its governance is contributing to the delivery of its strategy. | Trust is an active system member. The Deputy CEO/Medical Director is a member of the ICB Board. The Chair is a member of the NENC ICS Chairs Network. The CEO is a member of the NENC Provider Collaborative. The Trust is an active member of the North East and North Cumbria Mental Health, Learning Disability and Autism Partnership Provider Collaborative. The Executive Director of Finance is Chair of the NENC MHLDA Partnership Board. |
•Board reports •Board minutes • Finance Reports • Committee reports to Board • Annual report |
| Section A 2.3 | The board of directors should assess and monitor culture. Where it is not satisfied that policy, practices, or behaviour throughout the business are aligned with the Trust’s vision, values, and strategy ‘With you in mind’ strategy, it should seek assurance that management has taken corrective action. The annual report should explain the boards activity and any action taken, and the trust’s approach to investing in, rewarding, and promoting the wellbeing of its workforce. | The Board through its committees review data on the National Staff Survey, quarterly pulse surveys and Freedom to speak up concerns. The Trust has established a People Committee with responsibility for oversight of key workforce issues including wellbeing of the workforce. The Board of Directors oversees the Board Assurance Framework (BAF) which includes a high-level risk for the Trust associated with ensuring a focus on wellbeing of the workforce. All members of the Board are engaged in a programme of service visits as an opportunity to speak to staff. The Trust also undertakes regular engagement with staff, service visits and monthly Exec Q&A sessions. |
• Board reports • Board Minutes • Integrated Performance Report • Committee Reports • Staff Survey report and action plans • Staff Networks • FTSU process • Service visit feedback • Exec Q&A attendance • Thrive website • Annual report |
| Section A 2.8 | The board of directors should describe in the annual report how the interests of stakeholders, including system and place-based partners have been considered in their discussions and decision making and set out the key partnerships for collaboration with other providers into which the trust has entered. The board of directors should keep engagement mechanisms under review so that they remain effective. | The Trust undertakes a significant amount of engagement work with stakeholders, partners, service users, carers, and the public to inform the development of the strategy. |
• Board reports |
| Section B 2.6 | The board of directors should identify in the annual report each non-executive director it considers to be independent. Circumstances which are likely to impair, or could appear to impair, a non-executive directors independence include, but not limited to, whether a director: • Has been an employee of the Trust within the last two years. • Has, or has had within the last two years a material business relationship with the trust either directly or as a partner, shareholder, director, or senior employee of a body that has such a relationship with the Trust. • Has received or receives renumeration from the trust apart from a director’s fee, participates in the trust’s performance-related pay scheme or is a member of the trusts pension scheme. • Has a close family ties with any of the Trusts advisers, directors, or senior employees. • Holds cross-directorships or has significant links with other directors through involvement with other companies or bodies. • Has served on the Trust board for more than six years from the date of their appointment. • Is an appointed representative of the Trusts university medical or dental schools. Where any of these or other relevant circumstances apply, and the board of directors nonetheless considers that the non-executive director is independent it needs to be clearly explained why. |
The Board considers all Non-Executive Directors to be independent. An up-to-date register of interests is maintained and published. Each Board and Committee meetings receive a register of Board members and seeks to identify and where appropriate record any conflicts. An annual Fit and Proper Persons Test aligned to the new Framework 2023 is undertaken and reported to NHS England. |
• Recruitment and appointment process for NEDs • Published register of interest on the website • Declaration of interest report to board and committees • Council of Governors minutes • Annual review of compliance report and minutes quality • Annual Report • FPPT process |
| Section B 2.13 | The responsibilities of the Chair, Chief Executive and Senior Independent Director if applicable, board and committees should be clear, set out in writing and agreed by the board of directors and publicly available. The annual report should give the number of times the board and its committees met and individual director attendance. | The roles of the Chair, Chief Executive and Senior Independent Director are detailed in the Trust Constitution which is publicly available. Each Annual Report details the number of times the Board and Committees have met and the individual attendance of Directors |
• Trust Constitution • Trust Annual Report • Board and Committee minutes • Job descriptions and recruitment processes |
| Section B 2.17 | The board of directors should meet sufficiently regularly to discharge its duties effectively. A schedule of matters should be reserved specifically for its decisions. For Foundation Trusts, this schedule should include a clear statement detailing the roles and responsibilities of the Council of Governors. This statement should also describe how any disagreements between the council of governors and the board of directors will be resolved. The annual report should include this schedule of matters or a summary statement of how the board of directors and the council of governors operate, including a summary of the types of decisions to be taken by the Board, the Council of Governors, Board Committees and the types of decisions which are delegated to the Executive Management of the Board of Directors. | The Board of Directors meets eleven times a year either through Board of Director meetings (Closed and Open) and Board Away / Board Development Days. The Trust Constitution and Scheme of Delegation details the matters reserved for the Board, Council of Governors and those delegated to Committees. The Constitution sets out how any disputes between the Board and Council of Governors should be resolved. |
• Board Reports • Board Minutes • Council of Governor minutes • Scheme of Delegation • Trust Constitution • Board Cycle • Annual Report |
| Section C 2.5 | Open advertising and advice from NHS England’s Non-Executive Talent and Appointments team is available for use by nominations committee to support the Council of Governors and/or independent members in the majority. If an external recruitment agency is engaged, it should be identified in the annual report alongside a statement about any other connection it has with the Trust or individual directors. | The Board and Council of Governors have accessed expertise from NRG Recruitment when recruiting to some Board posts. If appropriate, the Annual Report will detail when external recruitment agencies are engaged. |
• Recruitment and appointment process for NEDs • Nominations and Remuneration Committee and minutes • Annual report |
| Section C 2.8 | The annual report should describe the process followed by the Council of Governors to appoint the Chair and Non-Executive Directors. The main role and responsibilities of the Nominations Committee should be set out in publicly available written terms of reference. | The role of the two Committees responsible for the appointment of the Executive and Non-Executive (including the Chair) are clearly defined and detailed in their Terms of Reference. Their respective terms of reference of the committees are approved by the Board of Directors / Council of Governors. |
• Nominations and Remuneration Committees • Board reports and minutes |
| Section C 4.2 | The Board of Directors should include in the annual report a description of each director’s skills, expertise, and experience. Alongside this, the Board should make a clear statement about its own balance, completeness, and appropriateness to the requirements of the Trust. Both statements should also be available on the Trust’s website. | The Annual Report provides a description of each Directors experience and expertise as does the Trust’s website. A statement regarding how the Board ensures it is balanced and meets the requirements of the Trust is also included in the Annual Report. |
• Board reports • Board minutes • Annual report |
| Section C 4.13 | The annual report should describe the work of the nominations committee including: • The process used in relation to appointments, its approach to succession planning and how both support the development of a diverse pipeline. • How the board has been evaluated, the nature and e tent of an e ternal evaluator’s contact with the board of directors and individual directors, the outcomes and actions taken and how these have or will influence board comparison • The policy on diversity and inclusion including in relation to disability, its objectives and linkage to the trust vision, how it has been implemented and progress on achieving the objectives. • The ethnic diversity of the board and senior managers, with reference to indicator nine of the NHS Workforce Race Equality Standard and how far the Board reflects the ethnic diversity of the trust’s workforce and communities served. • The gender balance of senior management and their direct reports. |
The role of the two committees responsible for the appointment of the Executive and Non-Executive (including the Chair) are clearly defined in their Terms of Reference. Their respective terms of reference of the committees are approved by the Board of Directors and Council of Governors. |
• Nominations and Remuneration Committee Terms of Reference • Board Reports and minutes • Council of Governor reports and minutes. • Annual report |
| Section C 5.15 | Foundation Trust Governors should canvass the opinion of the Trusts members and the public, and for appointed governors the body they represent on the NHS Foundation Trusts for forward plan, including its objectives, priorities and strategy and their views should be communicated to the board of directors. The annual report should contact a statement as to how this requirement has been undertaken and satisfied. | In 2023 the Trust sought the opinion of stakeholders, the public and communities when developing its strategy ‘With you in mind’. The Trust seeks the opinion of all stakeholders including service users and carers every year in the development of its quality priorities. Alongside the Trust has an annual plan which specifically details objectives for the year aligned to the strategy. This is discussed with the Governors and consulted. The Trust has in place a bi-monthly e-newsletter to members which includes updates from members of the Council of Governors. |
• Board reports • |
| Section D 2.4 | The annual report should include: • The significant issues relating to the financial statements that the audit committee considered and how these issues were addressed. • An explanation of how the Audit Committee (and/or auditor panel for an NHS Trust) has assessed the independence and effectiveness of the external audit process and its approach to the appointment or reappointment of the external auditor, length of tenure of the current audit firm, when a tender was last conducted and advance notice any retendering plans. • An explanation of how auditor independence and objectivity are safeguarded if the external auditor provides non-audit services. |
The Audit Committee has responsibility for considering any significant issues and escalation to the Board. The responsibility is clearly defined in Committees Terms of Reference. The Audit Committee produces an annual report on its business which is included in the Trust Annual Report and submitted to the Board and shared with the Council of Governors. The Audit Committee has assessed the independence of the external audit process. The Trust undertook the reappointment of the external auditor 2023/24 through a tender process. |
• Audit Committee Terms of Reference • Board reports and minutes • Audit Committee reports and minutes • Council of Governors reports and minutes. • Audit Committee Annual report • Trust Annual Report • Minutes of the Council of Governors • External Auditor appointment process |
| Section D 2.6 | The directors should explain in the annual report their responsibility for preparing the annual report and accounts, and state that they consider the annual report and accounts, taken as a whole, is fair, balanced, and understandable, and provides the information necessary for stakeholders to assess the trusts performance, business model and strategy. | This is required statement to be signed by the CEO and Executive Director of Finance and are supported in signing this statement following scrutiny of accounts by the Audit Committee and Board. | • Board reports and minutes • Audit Committee Reports and minutes Annual report |
| Section D 2.7 | The board of directors should carry out a robust assessment of the trust’s emerging and principal risks. The relevant reporting manuals will prescribe associated disclosure requirements for the annual report. | The Trust’s Board Assurance Framework is reported to the Board of Directors and all Board Committee including the Audit Committee which has delegated responsibility for oversight of the Trust systems and processes for risk management. |
• BAF/CRR report to Board • EMG and BDG-Risk reports |
| Section D 2.8 | The board of directors should monitor the trust's risk management internal control systems and, at least annually, review their effectiveness and report on that review in the annual report. The monitoring and review should cover all material controls, including financial, operational and compliance controls. The board should report on internal control through the annual governance statement in the annual report. | The Board are supported in this by the Audit Committee and the development of the Annual Governance statement. The Annual Report requires Board approval. The Board and Board Committees receive the Board Assurance Framework/risk report on a quarterly basis. The Trust reviewed and approved the refresh of the Trust’s risk appetite, Risk Management Policy and approach to risk management during 2023/24. |
• Board reports and minutes • Audit Committee reports • Board committee reports • Audit Committee minutes • Annual Governance statement • Head of Internal Audit Opinion • Board Assurance Framework/risk reports • Annual Report |
| Section D 2.9 | In the annual accounts, the board of directors should state whether it considered it appropriate to adopt the going concern basis of accounting when preparing them and identify any material uncertainties regarding going concern. Trusts should refer to the DHSC group accounting manual and NHS foundation trust annual reporting manual which explain that this assessment should be based on whether a trust anticipates it will continue to provide its services in the public sector. As a result, material uncertainties over going concern are expected to be rare. | This decision is taken by the Audit Committee based on advice from Executive Director of Finance and External Audit. The decision is made taking into consideration the NHS England and Department of Health and Social Care guidance. The Audit Committee consider this in the preparation of the accounts and the final recommendation to Board. | • Board reports and minutes • Audit Committee reports and minutes • Annual Report |
| Section E 2.3 | Where a trust releases an executive director, e.g. to serve as a non-executive director elsewhere, the remuneration disclosures in the annual report should include a statement as to whether or not the director will retain such earnings. | Not applicable for this year. | • Appointment and remuneration Committee reports and minutes. • Annual Report |
Information, development, and evaluation
Reports from the Executive Directors, which include in-depth performance and financial information, are circulated to directors prior to every Board meeting to enable the Board to discharge its duties.
The Council of Governors receive regular presentations from the Executive Team and updates from Governors on the work of the Nominations Committee and working groups. On appointment or election, all Directors and Governors undertake an appropriate induction programme and are encouraged to keep abreast of matters affecting their duties.
Robust processes are in place for the annual appraisal of the Board of Directors. The Chair leads the NEDs in their appraisals and the Chief Executive leads the Executive Directors appraisals. The Chief Executive is appraised by the Chair. The Senior Independent Director leads on the Chair’s appraisal. The Board of Directors routinely reviews its performance and individual Committees self-assess their performance against their terms of reference annually.
Indemnities
In accordance with the Trust’s Constitution, as at the date of this report, indemnities are in place under which the Trust has agreed to indemnify its directors and Governors who act honestly and in good faith will not have to meet out of their personal resources any personal civil liability which is incurred in the execution or purported execution of their functions save where they have acted recklessly. Any costs arising in this respect will be met by the Trust.
Modern Slavery Act Statement
Introduction
Slavery and human trafficking remains a hidden blight on our global society. We all have a responsibly to be alert to the risks, however small, in our business and in the wider supply chain. Staff are expected to report concerns and management are expected to act upon them.
NTWS’ Modern Slavery Act Statement is available on www.
Statement on the Trusts commitment to Climate and Environmental Issues.
Our Trust Board declared a climate and ecological emergency in March 2020 and in April 2021 we published our first Green Plan setting out seven core commitments based on the principles of sustainable healthcare.
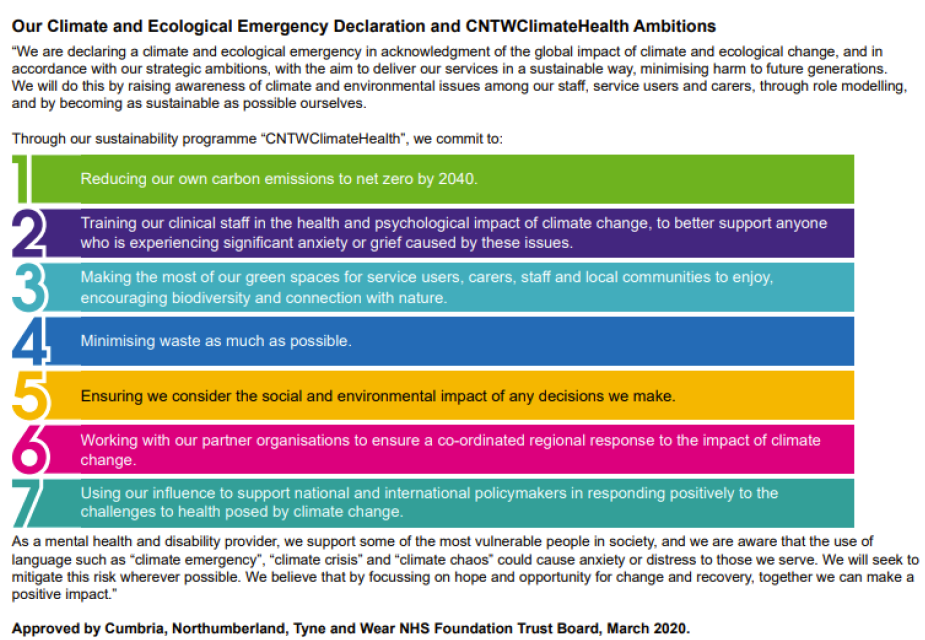
The principles of sustainable healthcare have also been incorporated throughout our Trust strategy, ‘With you in mind’ and the Trust Board-level Net Zero Lead is Kevin Scollay, Executive Director of Finance. Tacking the Climate Emergency is one of the priorities of focus in the NTW Solutions Ltd strategy and the NTW Solutions Board-level Net Zero Lead is Matthew Lessells, Director of Estates.
Our Carbon Targets
The NHS is a significant contributor to climate change, generating 4% of England’s total carbon footprint. In line with national targets and our own Green Plan, we must reduce the greenhouse gas emissions that result from the provision of our services to ‘Net Zero’. (Net zero is achieved when the amount of greenhouse gases produced, balance with the amount that's removed from the atmosphere. It can be achieved through a combination of emissions reduction and emissions removal).
Emissions are reported in tonnes of carbon dioxide equivalent (tCO2e), a figure that summarises all Greenhouse Gas (GHG) emissions with varying global warming potential (GWP) into a single carbon dioxide figure with the same global warming potential.
The source of the emissions determines whether they are reported within the Carbon Footprint (sources with the white background) or the Carbon Footprint Plus (all sources) in the figure below. The Trust has direct control over the emission sources within its Carbon Footprint and the ability to influence to additional sources included within the Carbon Footprint Plus.
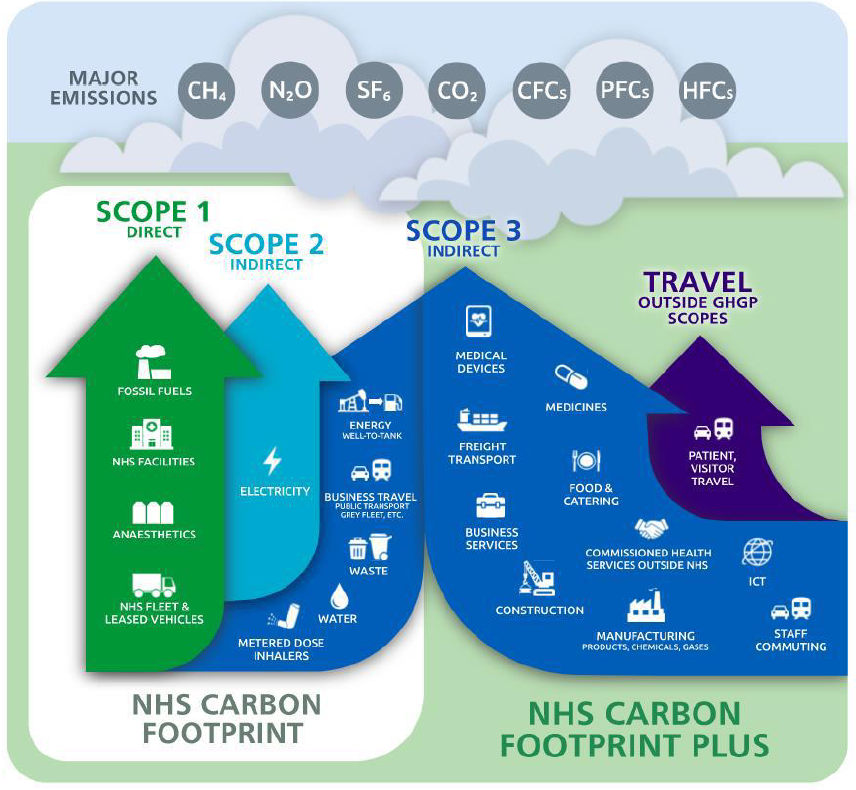
Based on these reporting boundaries, we have adopted the national NHS carbon targets:
•By 2040 our Carbon Footprint will be Net Zero
o With an interim target to reduce these emissions by 47% by 2028 to 2032 (compared to 2019/20 levels).
•By 2045 our Carbon Footprint Plus will be Net Zero
o With an interim target to reduce these emissions by 73% by 2036 to 2039 (compared to 2019/20 levels).
Our Carbon Performance
We monitor data for relevant emissions sources included within our Carbon Footprint. The following table and graph summarise CNTW’s annual carbon emissions by source, from our 2019/20 baseline year through to 2024/25.
| Emissions Source |
Annual Greenhouse Gas Emissions (tCO2e) 2019/20 |
2020/21 |
2021/22 |
2022/23 |
2023/24 |
2024/25 |
%change from 2019/20 | %change from 2023/24 |
|---|---|---|---|---|---|---|---|---|
| Fossil fuels | 5925 | 6179 | 5896 | 5574 | 5276 | 4997 | -16% | -5% |
| NHS Fleet & Leased Vehicles | 654 | 592 | 593 | 509 | 553 | 471 | -28% | -15% |
| Scope 1 Direct Sub-total | 6579 | 6771 | 6489 | 6083 | 5829 | 5468 | -17% | -6% |
| Electricity | 3284 | 2997 | 2847 | 2655 | 2845 | 2819 | -14% | -1% |
| Scope 2 Indirect Sub-total | 3284 | 2997 | 2847 | 2655 | 2845 | 2819 | -14% | -1% |
| Energy Well-to-Tank | 1547 | 1512 | 2069 | 1887 | 1804 | 1754 | 13% | -3% |
| Business Travel | 852 | 477 | 483 | 707 | 953 | 662 | -22% | -31% |
| Waste | 23 | 53 | 43 | 36 | 26 | 50 | 120% | 91% |
| Water | 238 | 207 | 75 | 80 | 76 | 70 | -71% | -7% |
| Scope 3 Indirect Sub-total | 2660 | 2250 | 2670 | 2710 | 2859 | 2536 | -5% | -11% |
| Carbon Footprint Total | 12,523 | 12,018 | 12,006 | 11,448 | 11,533 | 10.824 | -14% | -6% |
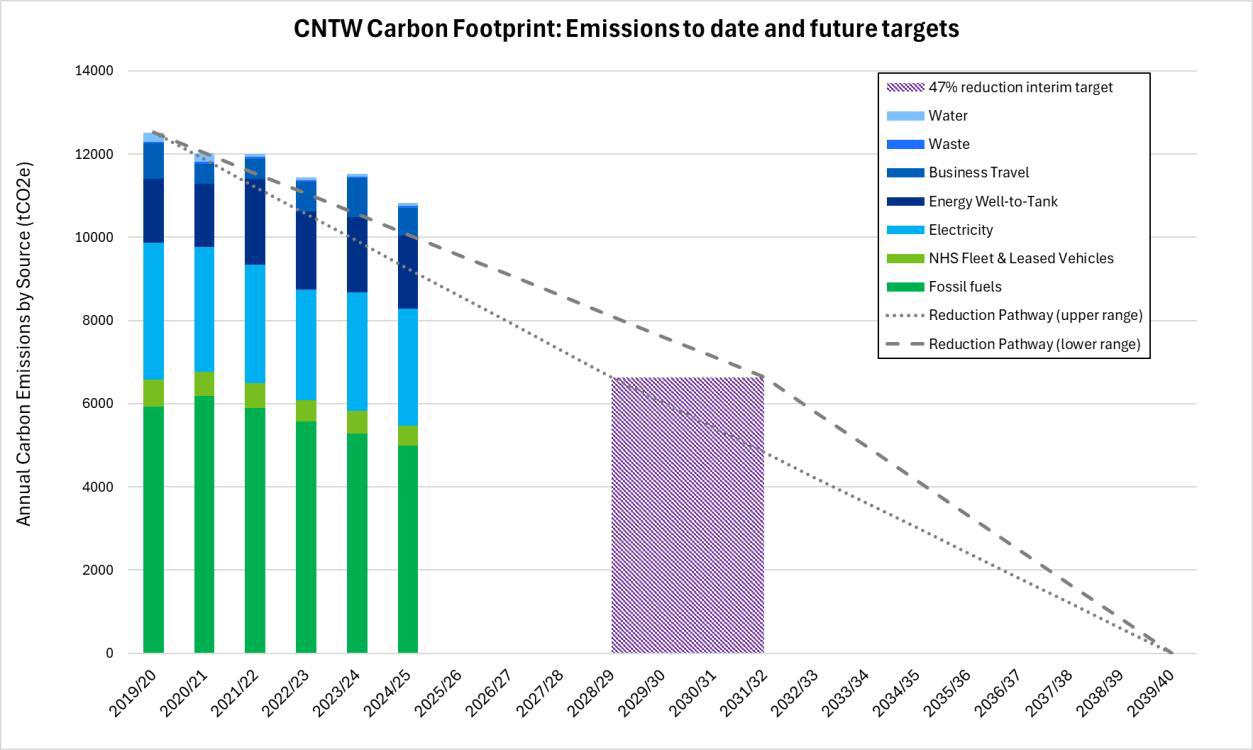
• In 2024/25 emissions from energy account for 88.4% of our Carbon Footprint
o We have reduced our emissions from fossil fuel use by 279 tCO2e compared to last year. Natural gas, use to heat our buildings and provide hot water, has reduced by 1,300 MWh (4.5%), and our use of gas oil for back-up generation has reduced by 157 MWh (76.8%).
o We have reduced our emissions from electricity by 26 tCO2e compared to last year. Electricity imported from national grid, used to power our buildings, and increasingly provide space heating and hot water, has reduced by 124 MWh (0.9%).
o We have reduced our indirect ‘well-to-tank’ emissions from energy by 50 tCO2e
(2.8%).
• In 2024/25 emissions from travel account for 10.5% of our Carbon Footprint
o We have reduced our emissions from fleet vehicles by 81 tCO2e (15%) compared to last year, by reducing our annual distance travelled by 473,816 miles.
o We have reduced our emissions from business travel by 291 tCO2e (31%) compared to last year, in part due to reducing our annual distance travelled by 32,890 miles.
•In 2024/25 emissions from waste processing and water supply and treatment account for 1.1% of our Carbon Footprint.
o Waste generated has reduced compared to last year, but more waste disposed via high temperature incineration cause emissions to increase by 24tCO2e.
o Water use increased compared to last year, but associated emissions reduced by 6 tCO2e, due to the national carbon intensity conversion factors decreasing for both water supply and treatment in 2024.
Overall, CNTW’s Carbon Footprint has decreased by 709 tCO2e in 2024/25 (6%), compared to the previous year. Our annual carbon emissions are now 14% lower than our 2019/20 baseline year.
This is progress in the right direction, but emissions remain higher than the steady reduction pathway for our Net Zero targets. We will need to accelerate our rate of decarbonisation to achieve the national target of a 47% reduction by 2032 at the latest. This is achievable and much of the sustainability progress made this year has laid strong foundations to increase our chances of success.
Delivering our Green Plan
Buildings and Infrastructure
Reducing carbon emissions associated with energy use across our estate is a key strand of our Green Plan and route to Net Zero. As highlighted above, both gas and electricity use has reduced compared to last year. This is the resulting benefit of previous investments in energy efficiency and heating control improvements alongside site rationalisation activities and capital schemes.
£240,000 of capital funding was specifically allocated to sustainability projects in 2024/25, with the majority of this spend on energy saving schemes. Loft insulation upgrades have been installed in multiple buildings across St Nicholas Hospital site, further LED lighting and building management system (BMS) heating control upgrades completed, and concept design work to de-steam St Nicholas Hospital site commissioned. This enabled us to submit a £4.85m capital funding application to the Public Sector Decarbonisation Scheme Phase 4, the outcome of which will be known in May 2025. If successful, this project will achieve a significant step towards decarbonising the site and replacing inefficient, ageing fossil fuel assets.
Securing additional capital funding is essential to decarbonise our estate. Demand is extremely high for national grant schemes, far beyond the available funding so we continue to focus on developing good projects and proactively bid for grants. In 2024/25 we submitted proposals for solar arrays at Northgate, St George's Park and Carleton Clinic for projects totalling £2.5m. Unfortunately, these bids were not successful and are on a reserve list should future funding be available. We did however successfully secure £820k of grant funding via the NHS Energy Efficiency Fund. This delivered large scale LED lighting upgrades across Walkergate Park and Carleton Clinic sites, BMS upgrades across sites in Cumbria and building-level sub-metering upgrades across multiple sites. Previous investment in Automatic Meter Reading (AMR) loggers on all water supplies has also enabled us to detect irregular water consumption patterns and act promptly to identify and resolve water leaks, avoiding unnecessary costs and carbon emissions through better management.
Waste and Resources
Our aim is to minimise waste as far as possible. Whilst waste only accounts for a small proportion of our carbon emissions, the appropriate segregation of waste streams is important to the Trust to maintain compliance, reduce costs and reduce the negative environmental impact of our healthcare activities. In 2024/25 we have made progress in the following areas:
• Renewed our general and recycling waste contract. Improving our recycling rate volumes remains an area for improvement. We are working with our new waste contractor to develop improvement projects.
• Piloted the use of reusable sharps containers at Walkergate Park. This project was well received by clinical and operational colleagues and resulted in the reduction of single-use plastic waste. Reusable sharps containers have now been permanently adopted at this site, and we plan to replicate this approach across others suitable sites.
• Continued to use Warp-It to facilitate the internal reuse of furniture across our sites, reducing unnecessary procurement and waste generation, saving both carbon and costs.
Green Spaces and Biodiversity
Our estate benefits from fantastic green spaces. Making the best of these for our service users, carers, staff, and local communities is a key aim of our Green Plan. Increasing biodiversity is a great way to do this. In 2024/25 we have made progress in the following areas:
• Planted over 350 trees across six sites through the NHS Forest scheme.
• Conducted baseline ecological surveys across multiple sites, providing insights into current biodiversity levels and providing recommendations to improve ecological scores to implement over the coming years.
• Established multiple wildflower meadows to support pollinators.
• Designated areas for No Mow May to enhance biodiversity.
• Mapped existing green spaces and identified opportunities for enhancement.
• Developed a questionnaire to assess and improve the use of green spaces, supporting nature access for patients and staff while identifying both current and historical uses to guide future planning.
Supply Chain and Procurement
Procured good and services form the largest share of the NHS Carbon Footprint Plus. The national Greener NHS team has set a Net Zero Supplier Roadmap to help Trusts influence supply chains to support the NHS net zero target. Our current Green Plan was written before these national changes and doesn’t include specific objectives linked to our supply chain. However, we have been proactive in delivering our services in line with the national best practice and will formally incorporate this key area of work in our next Green Plan. In 2024/25 we have made progress in the following areas:
• Evolved the Procurement Plan in alignment with sustainability goals and stakeholder priorities. Social value continues to be considered on all strategic contracts with at least 10% allocated to the award criteria. We request all tendering suppliers confirm they will work towards the aims and objectives of the ‘Net Zero Supplier Roadmap’.
• Completed an analysis of Trust expenditure to estimate the scope 3 (indirect) carbon emissions resulting from the goods and services we have procured.
• Procured Smart Carbon software and initiated a project to evolve our initial carbon estimates to improve reporting accuracy, identify opportunities to deliver supply chain carbon and cost saving benefits and support ongoing best practice reporting.
Travel and Transport
Our carbon emissions from travel have reduced in 2024/25, due to a reduction in travel completed by our own fleet and via business travel. In 2024/25 we have made progress in the following areas:
• We have further decarbonised our existing fleet, replacing older fossil fuel vehicles. Currently 66% are ultra-low emission vehicles (ULEV) emitting less than 75g of CO2 per kilometre, with 41% being pure electric vehicles (EVs).
• Collaborating with other Trusts in the region, we are part of North East Combined Authority funded project to understand our staff commuting habits. We completed a staff travel survey in January and a repeat survey will be conducted next year. The project will help us understand the current preferred modes of travel for our staff, identify opportunities to encourage modal shifts to lower carbon travel options, work with NECA to identify public travel improvements that will help our staff, and inform interventions we can take to help reduce the carbon impact of staff commuting.
• Continuing work to support more active travel to promote the health and wellbeing benefits to our staff.
Future focus on developing travel plans for our sites will benefit from the developments made this year and help inform a Trust-wide travel strategy.
Medicines and Models of Care
With a lower carbon footprint than many other healthcare sectors, mental health and learning disability services have much to offer in taking a holistic approach to developing sustainable healthcare. CNTW have been a leader in championing this, being a founder member of the Green Minds Network, a collaboration of Mental Health and Learning Disability Trust staff who have an interest in sustainable healthcare. Unfortunately, progress in this area of focus within the Green Plan has slowed in 2024/25 due to key sustainability staff changes. Focus has necessarily shifted to engaging new colleagues across the Trust to support the Green Plan delivery under a revised structure. Despite these setbacks, there has been notable progress in staff-led engagement in 2024/25:
• Staff at Castleside Day Hospital formed a sustainability team to help reduce the environmental impact of their service while continuing to provide excellent care for patients. By discussing sustainability regularly at team meetings, they made multiple positive changes across the service, from replacing single-use to reusable items, encouraging colleagues to ‘think before you print’ and switch off lights and equipment to save energy, utilising the Warp-it systems, and by welcoming crews from North East Ambulance Service into the building so that ambulance engines don’t need to be left idling, helping NEAS reduce their fossil fuel use and benefit buildings users by reducing local air pollution.
• Pharmacy Teams have developed a ‘Return for Reuse’ project which aims to avoid unnecessary medicines waste, saving resources and costs. This will be rolled out in the year ahead, alongside plans to review and reduce travel emissions associated with pharmacy services across the Trust.
Staff training and Engagement
We have consistently shared sustainability updates with our staff throughout the year, with the aim of increasing the visibility of the Green Plan and our ongoing commitment to embed sustainability throughout the Trust. Highlights include:
• Regular sustainability-related articles in staff newsletters
• Updated sustainability information on our intranet and websites
• Regular social media updates
• Relaunched the Green Plan Microsoft Teams channel with renewed staff engagement
Members of the NTWS leadership team have also completed the ‘Building a Net Zero NHS’ online training and other staff within NTWS have been encouraged to complete this too. We intend to increase uptake of this useful introductory training to a wider staff audience going forward and promote other sustainability training available.
Workforce and Leadership
Following the establishment of a new Green Plan delivery structure last year, progress has been made in 2024/25 to mature our dedicated sub-groups covering the key areas of work of Estates and Facilities, Travel, Supply Chain and Communications, with regular meetings held to coordinate more joint working on sustainability projects than before. Efforts to link in additional colleagues for other key areas of work including Digital Transformation, Medicines and Food and Nutrition has also been made. All groups feed into the now well-established Green Plan Management Group to track overall progress towards our Green Plan commitments, reported onwards to both NTW Solutions and CNTW Boards.
Partnerships, particularly as part of North East North Cumbria Integrated Care System Provider Collaborative and via national and regional networks, have strengthened over the last year. CNTW has active representation at various sustainability leads forums, working collaboratively with other Trusts to share best practice and collectively increase sustainability knowledge, skills, and capacity across the system.
Task Force on Climate-Related Financial Disclosures (TCFD)
NHS England’s NHS foundation trust reporting manual has adopted a phased approach to incorporating the TCFD recommended disclosures as part of sustainability reporting requirements for NHS bodies, stemming from HM Treasury’s TCFD aligned disclosure guidance for public sector annual reports. TCFD recommended disclosures as interpreted and adapted for the public sector by the HM Treasury TCFD aligned disclosure application guidance, will be implemented in sustainability reporting requirements on a phased basis up to the 2025/26 financial year. Local NHS bodies are not required to disclose scope 1, 2 and 3 greenhouse gas emissions under TCFD requirements as these are computed nationally by NHS England.
The phased approach incorporates the disclosure requirements of the governance, risk management and metrics and targets pillars for 2024/25.
Governance
The CNTW Board of Directors are responsible for oversight of climate related risks and opportunities. Our Green Plan 2021-2026 was approved by the Board in April 2021, which sets out the strategic direction and objectives of the Trust regarding sustainability and climate related issues.
The Executive Director of Finance is the CNTW Net Zero Lead with overarching responsibility for the management of climate and environment issues, supported by the Director of Estates as the Net Zero Lead for NTW Solutions. Operational implementation of the Green Plan is overseen by the Green Plan Management Group, which reports to the BDG Finance and Executive Management Group, onwards to Trust Board, and NTW Solutions Leadership Team and onwards to NTW Solutions Board.
Risk Management
Climate related risks are identified, assessed, managed and reported via the governance structure described above. The risk is currently scored as 12, which is classed as a moderate risk and is monitored via our directorate risk management process. The main climate related risks identified by the Trust are related to staff resource to coordinate the successful delivery of the Green Plan and the availability of sufficient capital funding to deliver decarbonisation projects at the speed and scale required to meet Net Zero targets.
Metrics and Targets
The Trust reports its carbon performance as a reduction against a baseline year of 2019/20, with supporting key performance indicators linked to the driving data behind this, including energy consumption, waste generated, water use, and distance travelled.
Metrics and measurements are reported annually within the Estates Return Information Collection (ERIC) with kWh/m2 for energy, m2 / m3 for water, kg / m2 for waste, % of LED coverage and number of heat or flood events that triggered a risk assessment.
Statement of the chief executive's responsibilities as the accounting officer of Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust
The NHS Act 2006 states that the Chief Executive is the accounting officer of the NHS Foundation Trust. The relevant responsibilities of the accounting officer, including their responsibility for the propriety and regularity of public finances for which they are answerable, and for the keeping of proper accounts, are set out in the NHS Foundation Trust Accounting Officer Memorandum issued by NHS Improvement.
NHS Improvement, in exercise of the powers conferred by Monitor by the NHS Act 2006, has given Accounts Directions which require Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust to prepare for each financial year a statement of accounts in the form and on the basis required by those Directions. The accounts are prepared on an accruals basis and must give a true and fair view of the state of affairs of Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust and of its income and expenditure, other items of comprehensive income and cash flows for the financial year.
In preparing the accounts and overseeing the use of public funds, the Accounting Officer is required to comply with the requirements of the Department of Health Group Accounting Manual and in particular to:
• Observe the Accounts Direction issued by NHS Improvement, including the relevant accounting and disclosure requirements, and apply suitable accounting policies on a consistent basis.
• Make judgements and estimates on a reasonable basis.
• State whether applicable accounting standards as set out in the NHS Foundation Trust Annual Reporting Manual (and the Department of Health and Social Care Group Accounting Manual) have been followed and disclose and explain any material departures in the financial statements.
• Ensure that the use of public funds complies with the relevant legislation, delegated authorities, and guidance.
• confirm that the annual report and accounts, taken as a whole, is fair, balanced and understandable and provides the information necessary for patients, regulators and stakeholders to assess the NHS foundation trust’s performance, business model and strategy.
• Prepare the financial statements on a going concern basis and disclose any material uncertainties over going concern.
The accounting officer is responsible for keeping proper accounting records which disclose with reasonable accuracy at any time the financial position of the NHS foundation trust and to enable them to ensure that the accounts comply with requirements outlined in the above-mentioned Act. The Accounting Officer is also responsible for safeguarding the assets of the NHS foundation trust and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities.
As far as I am aware, there is no relevant audit information of which the foundation trust’s auditors are unaware, and I have taken all the steps that I ought to have taken to make myself aware of any relevant audit information and to establish that the entity’s auditors are aware of that information.
To the best of my knowledge and belief, I have properly discharged the responsibilities set out in the NHS Foundation Trust Accounting Officer Memorandum.
![]()
James Duncan
Chief Executive
25 June 2025
Scope of responsibility
As Accounting Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of the NHS Trust’s policies, aims and objectives, whilst safeguarding the public funds and departmental assets for which I am personally responsible, in accordance with the responsibilities assigned to me. I am also responsible for ensuring that the NHS Trust is administered prudently and economically and that resources are applied efficiently and effectively. I also acknowledge my responsibilities as set out in the NHS Trust Accountable Officer Memorandum.
The purpose of the system of internal control
The system of internal control is designed to manage risk to a reasonable level rather than to eliminate all risk of failure to achieve policies, aims and objectives; it can therefore only provide reasonable and not absolute assurance of effectiveness. The system of internal control is based on an ongoing process designed to identify and prioritise the risks to the achievement of the policies, aims and objectives of the Trust and the Group, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively, and economically. The system of internal control has been in place in Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust and the Group for the year ended 31 March 2025 and up to the date of approval of the Annual Report and Accounts.
Capacity to handle risk
The Director of Communications and Corporate Affairs has overall lead responsibility for risk management within the Trust. While the Director of Communications and Corporate Affairs has a lead role in terms of reporting arrangements, the Executive Director of Nursing, Quality Assurance and Therapies has Executive responsibility and all directors have responsibility for the effective management of risk within their own area of direct management responsibility, and corporate and joint responsibility for the management of risk across the organisation.
Structures and systems are in place to support the delivery of integrated risk management, across the organisation. Risk management training to support the implementation of the Risk Management Policy which includes a risk appetite framework, has continued to take place throughout the Trust this year. This includes training for new staff as well as training which is specific to roles in areas of clinical and corporate risk. During the year, the Trust implemented a new Risk Management e-learning package. The training has been made mandatory for all staff Band 7 and above where holding a risk register is an integral part of their role, and a required competency. This also applies to NTW Solutions staff.
Delivery of mandatory training against standards is monitored by the People Committee as part of the workforce performance report, through delegated responsibility from the Board of Directors (“the Board”). Oversight throughout the year is managed by the Executive Management Group and Business Delivery Group-Risk and Business Delivery Group-Workforce (for training standards), and devolved Care group structures. The Trust has a Board-approved Risk Management Policy and Risk Appetite in place.
Since 2023/24, the Trust has been through a period of significant change. This includes changes in the Trust’s leadership of the organisation not only changes to the Executive Team structure and portfolios, but also the appointment of a new Chair of the Council of Governors and Board of Directors and newly appointed Non-Executive Directors. The Trust recognises the implementation of Integrated Care Systems (ICS) and Integrated Care Boards (ICB) and Partnerships and the need to operate within a system that incorporates the NHS ICB structures. Alongside this, we have also made the following organisational changes:
• A review of, and implementation of, the Trust governance framework (during 2023/24 and into 2024/25).
• A review of, and implementation of, the Trust risk management systems, processes and policy during 2024/25.
• A review of, and implementation of, the Trust operational structures (implementation from April 2024)
Following a review of the Risk Management Policy and process during 2023/24, the new Risk Management Policy was launched in March 2024. Following the implementation of the Trust’s ‘With You in Mind’ strategy in 2023, all supporting strategies were withdrawn to enable a single strategy for the organisation to shape a clear direction, and culture. This included the withdrawal of the Risk Management Strategy.
The Board reviewed the Trust’s risk appetite in 2023 in the conte t of the above. It was agreed that the risk appetite for the Trust would reflect the inclusion of risks relating to digital, workforce, model of care and innovation. The appetite for financial risk has been re-evaluated from moderate to low and climate risk has also been re-evaluated from low to moderate. A further review of the Trust Risk Appetite Framework is scheduled to take place during 2025/26.
Alongside a review of the Trust’s risk appetite, the Board also undertook a review of the Board Assurance Framework (BAF) to consider the changing internal and external landscape and ensure the Board were focused on the key risks to the achievement of the organisation’s strategic objectives. This resulted in a substantial review of risks, the format and content of the BAF, and clarity on controls, mitigations, and actions.
Following this, a wholescale review of the Trust’s approach to risk management was undertaken and launched in March 2024. This included a substantial review of the risk management process, risk management policy and associated training and guidance for staff. This included learning from well led, and independent reports from other organisations into governance failures including how risks are managed across large and complex organisations.
Not only has the policy been reviewed in light of the changes to the risk appetite statement, but it was significantly amended to make the policy clearer and simpler in terms of how risks are managed and escalated from ward to board (and de-escalated from Board to ward) and where risks are reviewed and monitored to ensure that they are being managed at the most appropriate level within the organisation. The policy also reflects the implementation of the Corporate Risk Register (CRR) which reflects the highest scoring ‘operational’ risks within the organisation for Executive and Senior Management scrutiny and awareness. The Corporate Risk Register was implemented as part of BAF report to the Board and its Committees from quarter 4 2023/24, to provide additional assurance regarding escalation and de-escalation of high-level risks. The new risk management process, including the BAF and CRR has been in place throughout the 2024/25 year.
A comprehensive, easy to understand, e-learning package been developed. This is an interactive on-line e-learning package which incorporates a test of learning. In March 2024, a review of the Trust’s mandatory training requirement was reviewed. Awareness of the training is also regularly promoted within the Trust staff weekly bulletin to encourage take up of training for all staff across the organisation.
Committees of the Board are in place both to ensure effective governance for the major operational and strategic processes and systems of the Trust, and to provide assurance that risk is effectively managed. Operations for the Trust are managed through an organisational structure, with operations divided into three Care Groups (each of which has several clinical business units), and each has governance groups in place for quality, risk, finance, workforce and performance). Risk registers are maintained and reviewed by each Group and reviewed through the Trust-wide governance framework.
2024/25, two groups established during the 2023/24 year continued to operate which has fundamental responsibility for risk identification and escalation across the Trust. The Executive Management Group (EMG) review the CRR, the highest level operational risks across the organisation which require Executive level oversight, as well as all risks scoring an impact of 5 – major (regardless of likelihood score). EMG is comprised of Executive Directors and Director-level subject experts. BDG-Risk is comprised of Care Group and corporate leads and was implemented as a forum to discuss the Trust’s risk registers collectively and take an opportunity to sense-check how risks are being identified, scored, and controlled, particularly for those risks which are identified across more than one Care Group, or directorate. BDG-Risk provides a forum to discuss training needs relating to risk across the organisation and ensure consistency in approaches to risk management. A key responsibility of BDG-Risk is to undertake ‘deep dives’ on areas where risks may require a discussion and review across more than one area, or where the number of risks relating to specific issue are high for collective discussion and learning in terms of successful mitigations.
The Committees of the Board are required to consider the risks pertaining to their areas of responsibility by reviewing the management of risks documented in the BAF to receive assurance that effective controls are in place to manage these risks and to report any significant risk management and assurance issues to the Audit Committee and the Board.
The Audit Committee considers the systems and processes in place to maintain and update the BAF and wider risk management and internal control processes, it considers the effectiveness and completeness of assurances and that documented controls are in place and functioning effectively.
The risk and control framework
The Trust continually reviews its risk and control framework through its governance framework and operational structures. As described above, it has identified its major strategic risks, and these are monitored, maintained, and managed through the BAF, with delegated responsibility for risk management to the Audit Committee, and delegated responsibility for ongoing review and oversight of strategic risks via the Board Committee structure. Risk management is also supported by Corporate, Group/Directorate, Clinical Business Unit and ward/department risk registers. Outcomes are reviewed through consideration of the BAF, and all risk registers to assess for completeness of actions, review of the control mechanisms and on-going assessment and reviews of risk scores. Regular quality checks are undertaken by the Risk Management Lead on all closed risks, new risks, and risk reviews.
Internal Audit provides assurance on the management of key risks and the effectiveness of the Risk Management Framework and process, and BAF on an annual basis. The Risk Management process is evaluated by Internal Audit on compliance and areas of best practice focusing on the BAF and ensuring it is considered by the Board and Board Committees sufficiently as well as risks at all levels and that there is evidence that the risks are appropriately managed.
Due to the significant changes and improvements in the risk management processes during 2023/24, the Director of Communications and Corporate Affairs requested that two separate audits be undertaken. One on the BAF process and one on the wider risk management processes across the Trust. This was requested to provide additional assurance on the effectiveness of the new risk management processes, the embedding of the new process, and whether any improvements were required following year-one of launch.
The Trust received ‘substantial’ assurance through the internal audit process for 2024/25 relating to both the Board Assurance Framework audit and the risk management processes.
Risks facing the organisation are identified from several sources, for example:
| Proactive | Reactive |
|---|---|
| • Visual assessments, day to day work related tasks or activities. • Annual planning and objective setting • Performance monitoring and trends • Internal and external engagement and consultations with staff, service users and carers, and stakeholders • Integrated risk management self-assessment tool • Quality and other impact assessments of new developments, service reviews and cost improvement programmes • Mandatory/statutory standards. • National independent reviews • Horizon scanning and internal and external policy reviews • Benchmarking |
• Review of cases where things have gone wrong and has resulted in harm, incident or complaint • Review of cases where things have gone right and learning from best practice • Health and safety inspections, external visits, and reviews. • External decisions and recommendations impacting on the Trust • Audit outcomes (clinical, internal, and external) • CQC and other regulatory reports. • Shared learning from other organisations/professional bodies/forums (i.e., fire assessments, regional forums |
The Board, through its Risk Management Policy has adopted a risk appetite statement which shows the amount of risk the Board is willing to accept in seeking to achieve its strategic ambitions. The final risk appetite was agreed by the Board in January 2024. A further review of the Trust’s risk appetite will be undertaken during 2025/26 through an externally facilitated discussion.
Risk appetite is 'the amount and type of risk that an organisation is willing to take in order to meet their strategic objectives’. The same risk appetite is applied to the assessment of risk across the organisation. The risk appetite allows the Trust to measure, monitor, and adjust, the actual risk positions against the risk appetite so people can focus on the level of attention a particular risk may need, whether a risk needs to be escalated for more senior oversight or intervention.
The Trust has a low tolerance to taking risks which may impact on service users, staff safety, effectiveness and experience, but are more willing to accept opportunity risks such as innovation, service developments and partnership working.
Risk is managed at the lowest level possible, as close to the source of the risk as possible. Risks that fall within the risk appetite scores should always be maintained on local risk registers and escalated as described above. On initial assessment, risks which score 1 – 5 are recorded on the on-line Web-risk system but are not transferred to the live risk registers. Decisions regarding the closure of risks will be made following discussion with the risk owner and their clinical/operational manager, with oversight being provided by the Risk Management Lead.
All risks which exceed the Trust’s risk appetite are reported through the Trust Governance framework as described above.
Board Assurance Framework (BAF)
The table below summarises those risks as reported to the Board in the BAF as of 31 March 2025. All risks identified below are considered as in-year and future risks relating to the achievement of the Trust’s strategic ambitions pertinent to 2024/25.
| Risk Ref | Risk Description | Risk Appetite | Risk Score (LXI) |
|---|---|---|---|
| 2510 | Due to increased demand the Trust is unable to meet regulatory standards relating to access, responsiveness, and performance resulting in a risk to quality and safety of patient care. | Quality safety (6-10) | 4x4 = 16 |
| 2511 | Risk of not meeting regulatory and statutory requirements of Care Quality Commission (CQC) registration and quality standards. | Quality effectiveness/ experience (6-10) | 3x5 = 15 |
| 2512 | Risk of failing to maintain a positive patient safety learning culture resulting in avoidable harm, poor systems, process and policy, and escalation of serious issues of concern. | Quality safety (6-10) | 3x4 = 12 |
| 2542 | Failure to develop a sustainable workforce model to recruit/retain/ and support the development of the right people with the right skills to deliver safe and effective services, our strategic objectives, and contractual obligations. | Workforce/ staffing (6-10) | 4x4 = 16 |
| 2544 | Risk of poor staff motivation, engagement, and job satisfaction if issues affecting staff experience are not addressed including health and wellbeing support, inclusion and the ability to speak up. | Workforce/ staffing (6-10) | 3x4 = 12 |
| 2545 | Failure to deliver a sustainable financial position and longer-term financial plan, will impact on Trust’s sustainability and ability to deliver high quality care. | Financial (6-10) | 4x4 = 16 |
| 2547 | Risk that the Trust’s information and systems is at higher risk of being compromised leading to unknown vulnerabilities. This could lead to loss of, and/or public disclosure of, information and loss of access to critical systems. | Digital-cyber threats (6-10) | 3x4 = 12 |
| Risk Ref | Risk Description | Risk Appetite | Risk Score (LXI) |
|---|---|---|---|
| Risk 2543 | Failure to deliver our transformation plans around the model of care which affects the quality and sustainability of services. (is not currently breaching the risk appetite) |
Model of Care (12-15) | 3x4 = 12 |
The following details risk scores were reduced during the year for risks held on the Board Assurance Framework and were de-escalated to the relevant Directorate risk register.
| Risk Ref | Risk Description | Risk Appetite | Previous risk score | Current risk score |
|---|---|---|---|---|
| 2548 | If the Trust does not consider its own position as a 'good partner', and the position of others as capable of working in partnership, there is a risk that the Trust and the system does not allocate resource effectively, in the right place with the right organisations and partnerships which may impact on the ability to deliver high quality, safe services across the system. |
Partnership working (16-25) |
3x4 = 12 | 2x4 = 8 |
| 2541 | Risk that the Trust does not deliver the objectives of its Green Plan affecting the physical and mental health of current and future generations. | Climate and ecological sustainability | 4x5 = 20 | 4x3 = 12 |
| 2540 | Risk of increased staffing costs from use of temporary staff impacting on quality of care and financial sustainability | Financial (6-10) | 3x4 = 10 | 2x4 = 8 |
The Trust engages and involves stakeholders in identifying and managing risks to its strategic objectives in a number of ways. These include:
• The Trust is a key partner withing the North East and North Cumbria Integrated Care System, and has a strong relationship with the Integrated Care Board. The Trust is fully engaged in system-wide discussion both at Board level (Chair, Chief Executive and Executive networks) as well as place-based level through the localities. The Trust’s Deputy Chief Executive/Medical Director is also a member of the NENC Integrated Care Board as a partner representative.
• Working with partners in health and care services in considering business and service change. The Trust has a framework for managing change to services agreed as part of its contracts with its main commissioners across the Northeast and North Cumbria. The Trust also has strong relationships with Health Overview and Scrutiny Committees, with an excellent record of engagement and consultation in significant service change.
• Active relationships with community, voluntary and third sector organisations.
• The Director of Communications and Corporate Affairs reports directly to the Chief Executive and Chair for sustaining effective relationships with the key public stakeholders. The role is also a member of the Executive Director Team.
• Active engagement with the Trust’s own Service User and Carer Reference Group. The Group is comprised of more than 100 service users and is chaired by a carer.
• Active engagement with the Council of Governors on strategic plans, service change, quality, and safety risks, including active engagement in the preparation of the Annual/Forward plan, service changes, and the setting of Quality Priorities.
The involvement of public and e ternal stakeholders in the Trust’s management of risk management involves timely communication, engagement, involvement, and consultation, where necessary. We ensure good communication both internally and externally is included as a key consideration for any service change, service development, and our work on transformational change through our key programmes of work. This includes seeking their views on potential areas of risk and how risks are being managed.
The Trust reviews its governance arrangements on a regular basis and in particular risks associated with statutory and regulatory compliance. Such risks may include lack of clarity and effectiveness of governance structures, unclear reporting lines/ accountabilities between the Board, its committees and the executive leadership team; delay and ineffective scrutiny and oversight by the Board as a result of inaccurate and delayed information for Board and committee decision-making; and insufficient capability at Board level to provide effective leadership and challenge.
Governance and Performance Management
The Trust has a robust process in place to ensure all executive and non-executive directors are able to discharge their functions effectively with clear governance structures in place. Each has a distinct role around governance or performance management and provides opportunities for Board members at executive and non-executive level to review in detail the key risks, and data and information associated with the management of those risks, and actions being taken to mitigate them. All Committees also include representation from the Council of Governors to ensure a patient and public perspective on Trust business, scrutiny and challenge.
The Board receives information at every meeting relating to progress on performance, finance, workforce and quality, and additional metrics associated with service user and carer experience. The Integrated Performance Report provides these metrics, data and narrative and has been subject to review throughout 2024/25 to ensure robust data quality that provides appropriate assurance to the Board and promotes scrutiny and challenge.
As part of performance management, developing a sustainable workforce plan is a key aim within the Trust priorities for 2025/26. In line with the NHS Long Term Workforce Plan and associated People Plan, the Trust continues to re-energise its workforce planning methodology to move from short term workforce planning (up to 12 months) to medium term and eventually to longer term (5 years) to support clinical business units meet their strategic objectives. To support the workforce planning process several tools are available to stakeholders as well as the use of internal and external data.
Our integrated approach to workforce planning continues to be a golden thread through our transformation work. One example is community transformation, which has included a full skills analysis captured on the Electronic Staff Record across 7 pioneer teams. This work continues and will begin to develop medium to long term staffing plans and will inform further work which will begin on a wider scale.
The overall Trust Workforce Plan is incorporated into the annual planning cycle and formally reviewed by the Board on an annual basis. Regular establishment reviews take place as part of the safer staffing approach across the Trust and in response to wider workforce, quality and financial analysis. The Trust monitors and triangulates a full suite of indicators and Safer Staffing reports are provided to the Quality and Performance Committee which include identified risks and mitigations, including workforce. Progress of performance is monitored through the Trust’s internal processes.
The Trust monitors and triangulates a full suite of indicators, of which workforce is included, to report progress on the performance of the organisation through the Trust’s performance and assurance processes, including the Workforce Performance Report to the People Committee.
Internal Audit
In preparing the Head of Internal Audit Opinion, weaknesses in control were identified in two final reports with limited assurance being issued during 2024/25: Mental Health Act S136 Place of Safety (this related to the 2023/24 plan and was issued after the final 2023/24 opinion) and Duty of Candor Follow Up.
Mental Health Act S136 Place of Safety
Key issues arising from this report included the need to:
• Conduct regular spot checks on the completion of Section 135/136 forms, including the client’s health record, and take necessary actions, such as appropriately escalating issues and providing targeted training, to improve compliance.
• Implement a system for the regular monitoring and review of progress notes to ensure joint risk assessments are accurately and consistently recorded. This could be integrated into routine supervision or establish as a dedicated quality assurance process.
• Conduct a thorough review of specific incidents where joint risk assessments were not conducted, such as in the cases of form 9364 and form 9597. Identify the reasons for the deviations and take corrective actions to prevent recurrence.
• Update the section 135/ 136 form to include the date and time of the assessment, as well as the outcome of the assessment.
Duty of Candour follow up
High priority recommendations were found relating to clarifying training requirements and the process steps, including meetings that must take place, records that should be completed and where those records are to be held within the policy and conducting comprehensive training sessions for staff on the updated policy, emphasising the importance of verbal or written apologies, involving nearest relatives in post-incident discharge planning, nominating contact persons, and offering appropriate support to affected individuals.
For both audits, appropriate action plans have been agreed with management to address the issues raised. From the Internal Audit review of the systems of internal control, as part of the Head of Internal Audit Opinion, they have provided overall good assurance for their draft opinion as of May 2025.
Performance and assurance (including quality and safety)
The Trust’s performance and assurance systems and processes support the presentation and analysis of information at Trust, group, service and team levels which enables the dissemination of performance information to the various levels of the organisation, including staff teams. Performance, quality, and safety updates are also shared with the Council of Governors as well as the Board. To further enhance this, several quality dashboards have been developed throughout the year. Clinical dashboards enable clinical teams to monitor and review their performance and individual members of staff can also access their own personal dashboard which includes workforce and training information.
The Trust has published on its website an up-to-date register of interests, including gifts and hospitality, for decision-making staff, as required by the Trust’s Constitution and in line with NHS England guidance for managing conflicts of interest. The Trusts Declaration of Interest policy was last reviewed and approved by the Audit Committee in November 2024 with the next review scheduled to take place in 2027. The register of interests for the Board, Council of Governors and decision-making staff is available on the Trust’s website.
As an employer with staff entitled to membership of the NHS Pension Scheme, control measures are in place to ensure all employer obligations contained within the Scheme regulations are complied with. This includes ensuring that deductions from salary, employer’s contributions and payments into the Scheme are in accordance with the Scheme rules, and that member Pension Scheme records are accurately updated in accordance with the timescales detailed in the Regulations.
In addition, to ensure compliance with Developing Workforce Safeguards, the high level Trust Workforce Plan is incorporated into the annual planning cycle and formally reviewed by the People Committee on an annual basis. Regular establishment reviews (including new roles) take place, as part of the safer staffing and Developing Workforce Safeguards approach across the Trust and in response to wider workforce, quality and financial analysis.
Control measures are in place to ensure that all the organisation’s obligations under equality, diversity and human rights legislation are complied with. The Trust used the findings from the last equality delivery system assessment to inform the development of the Trust Equality Diversity and Inclusion Objectives approved by the Board in 2024 and a further review is scheduled to take place in April 2025. These will be reviewed and monitored through the Board appraisal processes year-on-year.
The Trust has undertaken risk assessments on the effects of climate change and severe weather and has developed a Green Plan following the guidance of the Greener NHS programme. The Trust ensures that its obligations under the Climate Change Act and the Adaptation Reporting requirements are complied with and further information on progress against the Trust Green Plan can be found in section 2.9, Sustainability Report within the Annual Report and Accounts. Risks associated with Climate and Ecological Sustainability was included in the Trusts risk appetite and the Board Assurance Framework includes a risk in relation to the impact of climate change. This risk was de-escalated in 2024 to Directorate level. The Trust has undertaken risk assessments on the effects of climate change and severe weather and has developed a Green Plan following the guidance of the Greener NHS programme. The trust ensures that its obligations under the Climate Change Act and the Adaptation Reporting requirements are complied with.
The Trust supports an open reporting culture and encourages its staff to report all incidents through its internal reporting system. The Trust’s Incident Policy CNTW(0)05 and supporting practice Guidance Notes provides the framework for staff for the reporting, management investigation and dissemination of lessons learnt.
The Patient Safety Incident Response Framework (PSIRF) sets out the new NHS approach to developing and maintaining effective systems and processes for responding to patient safety incidents for the purpose of learning and improving patient safety. The Trust had its Patient Safety Incident Response Plan (PSIRP) and Policy approved by the ICB and Trust Board in November 2023. In January 2024 the Trust started its implementation of PSIRF. Compliance with PSIRF has been ongoing and subject to assurance review by the Quality and Performance Committee, with any issues of concern escalated to the Board via the Committee assurance and escalation reporting process. The Trust safety framework includes levels of incident review:
• Early Learning Review (ELR) – completed within 7 days from request and identifies local actions to address safety concerns and identifies process and systems that might need exploration via an After-Action Review.
• After Action Review (AAR) – facilitated reflective review comprised of a group of clinical and operational staff involved in the provision of care for the service user (this can include a multi-disciplinary approach i.e., CNTW and external partners). The AAR will explore aspects of work within the services involved in care delivery, focusing on work ‘as done’ verses work ‘as imagined’. Completed within 60 days of request.
• Patient Safety Incident Investigation (PSII) – in-depth review of a single patient safety incident, or cluster of incidents to understand what happened and how. Conducted to identify underlying system factors that contributed to an incident. Completed within 90 days of request.
During 2023/24, levels of violence and aggression against staff increased, particularly within the specialist autism inpatient service provided at the Mitford Unit. Mitford provides a specialist autism inpatient service Concerns were raised by staff to the Health and Safety Executive (HSE) who carried out a targeted visit to the service in January 2024. In February 2024, the Trust was issued with an Improvement Notice by the HSE due to concerns about the levels and frequency of assaults on staff from patients. The Trust formally responded to this within the timeframes stipulated by the HSE. Work remains ongoing with the HSE and across the Trust in the context of the prevention and management of violence and aggression. Reduction in levels of violence and aggression continued throughout 2024/25 as one of the Trust’s Quality priorities, and is reported via the Quality and Performance Committee.
The Trusts governance framework is supplemented by an on-going programme of service visits by Executive Directors, Non-Executive Directors, and members of the Council of Governors. The feedback is shared with the Executive Team, to address any areas for action, and the Council of Governors for assurance purposes. To provide additional assurance, a comprehensive report has been developed, outlining the themes from all service visits and detail on the link of themes and issues to the Trust governance framework and risk management processes to ensure issues are being addressed appropriately. The report is reported to the Quality and Performance Committee who will use the intelligence from visits to identify any gaps in oversight, risks, reporting and controls across the Trust.
Care Quality Commission registration
Registration compliance is managed through the Trust’s Equality governance structures. The outputs of CQC inspections (themed reviews), CQC Mental Health Act Reviewer visits and internal peer review visits are all considered by the Trust CQC Quality Compliance Group as a means of ensuring shared learning and development across all service areas. We also seek assurance that these findings and associated actions are managed within the appropriate Care Group governance groups. The CQC Compliance Group reports to the Executive Management Group and Quality and Performance Committee.
The Trust is fully compliant with the registration requirements of the CQC and has maintained full registration, with no non-routine conditions, from 1st April 2010. The CQC conducted a Well Led review inspection during 2018 and rated the Trust as ‘Outstanding’. As part of CQCs well led review inspection during 2018 the trust governance arrangements came under further e ternal scrutiny. The Trust achieved an ‘Outstanding’ rating for Well-led in addition to its overall rating.
During July the CQC conducted an assessment of all wards for people with a learning disability or autism. Three locations were visited across two Care Groups, Mitford Unit, Northgate Park, Rose Lodge and Edenwood, Carleton Clinic. This core service was last inspected during 2022 and included some of the secure services at Northgate Park. On this occasion CQC decided against including Tyne and Tweed wards as part of this assessment and agreed to consider those wards as forensic or secure core services as part of a future inspection / assessment visit.
The CQC revisited the three-learning disability and autism wards on 12 September to check on the progress of improvement which the service was told to make following the July inspection. Following their revisit CQC felt assured that the Trust had a robust plan that the concerns have been or are in the process of being addressed. The Trust also continues to provide monthly reports to CQC to show further improvements which are being made to keep people safe.
The draft report from this assessment was received on 10 March 2025 and as of 31 March 2025, the final report was yet to be received. The final report when received will be available on the Trust’s website and reporting will be monitored through the CQC Compliance Group and Quality and Performance Committee.
In February 2025, the CQC conducted a focused inspection of community mental health and early intervention in psychosis teams. As of 31 March 2025, the draft report was yet to be received. The final report when received will be available on the Trust’s website and reporting will be monitored through the CQC Compliance Group and Quality and Performance Committee.
Governance Framework
During 2023/24, the Trust’s governance framework was the subject of internal review, led by the Director of Communications and Corporate Affairs. Changes made to the governance framework included the establishment of the Trust wide Leadership Forum (150+ leaders), establishment of the Executive Management Group, review of Business Delivery Group meetings, clarity of strategic, assurance and decision-making forums in terms of purpose and outcomes, and a reset of the Board of Directors and Council of Governors meetings, structures and cycles of business.
The Board governance structures are the subject of periodic review, the last review taking place December 2023. The outcome of the next review will be reported to the April meeting of the Board.
During quarter 3 2024/25, the Trust commissioned an external review of the governance framework, and other key elements of the well led framework. ConsultOne were commissioned to undertake the review.
The review was commissioned in the context of the changes within the Trust and its leadership during the previous 12-24 months, and changes to the governance framework and test the effectiveness of this in the context of being well led. The Trust sought an external perspective over three aspects of its governance arrangements to test:
• Board and committee governance, effectiveness, and ways of working (it was agreed that the Council of Governors would be excluded from this element as it was felt that this forum had recently been reviewed and subject to new ways of working and is operating effectively).
• Embeddedness of the Trust’s ‘With you in mind’ strategy and plans to deliver this.
• Executive effectiveness with a focus on understanding and appropriateness of the executive director responsibilities.
Each element of the review was subject to a separate report, recognising the different audiences and participation. The review included a broad range of activity including documentation review, one-to-one interviews, online survey, focus groups, meeting observations and research.
The outcome of the review was presented to the Board in February 2025 and overall, ConsultOne felt that the Board was in a good place with evidence of many areas of good practice. Feedback was positive including an improved position of Board diversity and a greater focus on Board development. They identified opportunities to strengthen the effectiveness and impact of the Board and for it to be more strategic and demonstrate greater ownership and ambition of its agenda. Refreshing and updating the Trust’s supporting strategies alongside greater specificity of outcome and measurement. Continuing improvements in the quality and focus of reporting including greater focus on assurance, escalation by exception and clarity of purpose and ask of reports.
The Board will review, oversee and monitor the outputs from the review during 2025/26.
Board committees
Each of the committees is chaired by a Non-Executive Director and has Executive Director Lead and Executive/Director membership. Each of the Board committees has responsibility for risks pertaining to their area of focus and ensuring the following takes place:
• Ensures that the Committee agenda reflects the key issues and risks facing the organisation and where focus needs to be maintained.
• Ensures a committee framework whereby Board Assurance Framework risks are reviewed with a specific focus on gaps in assurance to highlight and identify where escalation to Board is required.
• Review the Board Assurance Framework to ensure that the Board receives assurance that effective controls are in place to manage strategic risks.
• Receive assurance on the management of the Corporate Risks and alignment of these risks to the Board Assurance Framework.
• Report to the Board on any significant risk management and assurance issues.
The Audit Committee has operated as a key statutory committee of the Board with the responsibility for assuring the Board that effective processes and systems are in place across the organisation to ensure effective internal control, governance and risk management that support the achievement of the organisation’s objectives (both clinical and non-clinical). As part of the ConsultOne review of governance, overall, the Committee was found to be working effectively. There was also evidence of cross-committee working with opportunities to strengthen formalised and documented hand offs and retention of oversight, particularly clinical.
Internal Audit provides a regular review of financial procedures on a risk-based approach, and the outcomes of these reviews are reported to the Audit Committee. The Internal Audit Plan for the year is approved on an annual basis by the Audit Committee, and the Plan is derived through the consideration of key controls and required assurances as laid out in the Board Assurance Framework and individual discussions with Executive Directors and the Chair. The Audit Committee have received significant assurance on all key financial systems through this process.
The Mental Health Legislation Committee is a statutory Committee and has delegated authority to ensure that there are systems, structures, and processes in place to support the operation of mental health legislation, within both inpatient and community settings and to ensure compliance with associated codes of practice and recognised best practice. As part of the ConsultOne review, there was evidence of discussion, challenge and agreed actions however, further improvements are required in terms of this being reflected in the recording of the meetings. There was a recommendation for greater clarity on roles and responsibilities and flows of assurance between Board, committee and sub-groups.
The Remuneration Committee is a statutory committee of the Board and has responsibility for deciding and reviewing the remuneration, terms and conditions of office of the Trust Board Executive Directors and the Trust’s subsidiary companies, ensuring compliance with statutory and regulatory requirements.
The Quality and Performance Committee has responsibility for overseeing the Trust’s performance against fundamental standards for quality and safety. The Committee also considers all aspects of safety, quality and performance, clinical audit, and research. In common with the majority of Trusts, the ConsultOne review noted that the committee had a complex and broad remit. The committee was described as self-aware and knowledgeable of the required improvement areas. There was also evidence of completed, current, and planned action.
The Resource and Business Assurance Committee provides assurance that all matters relating to financial management, estates and infrastructure, digital innovation and technology, and business and commercial development are effectively managed and governed. The ConsultOne review noted the need to ensure that the committee has the capacity to accommodate its broad ranging coverage including financial, digital and provider collaborative.
The People Committee has responsibility for overseeing the delivery of the Trust’s Workforce strategy, programmes, and plans for delivery. The ConsultOne review, there was a recognised need to improve focus across the meeting agenda and an opportunity to widen contribution and influence.
Oversight of Quality Governance arrangements is achieved through the governance structures outlined above, ensuring there are arrangements in place from ward to Board. Review, monitoring, and oversight of these arrangements takes place through the following:
• Board of Directors.
• Quality and Performance Committee.
• Executive Management Group meetings.
• Trust wide Safety Group
• Business Delivery Group meetings (quality and performance, finance, workforce, risk).
• Care Group well-led meetings.
• Care Group operational management group meetings.
• Group quality standards meetings.
• Trust Leadership Forum.
Review of economy, efficiency and effectiveness of the use of resources
Annually, the Trust produces an Annual Plan which includes detailed plans for delivery of service and financial priorities for the year. A refresh of the overall Trust plan for 2024/25 was approved by the Board in April 2024 in line with national guidance. The financial position is reviewed monthly through BDG-Finance, bi-monthly, through the Executive Management Group meeting, and on a quarterly basis by the Resource and Business Assurance Committee (RABAC).
The Board receive regular updates on the financial position via updates from RABAC, the Integrated Performance Report and a separate Finance Board report. The Executive Management Group receive a bi-monthly report as well as specific updates on key issues, such as control of agency costs. Each Care Group reviews its own performance on its contribution to the Trust Financial Plan at its Care Group Operational Management Group. This is subject to review through monthly BDG-Finance meetings and quarterly well-led review meetings between Executive Directors and the Care Groups. The Trust actively benchmarks its performance, through a range of local, consortium based and national groups.
Information governance
The Trust has effective arrangements in place for Information Governance (IG) with performance against the Data Security and Protection Toolkit (DSPT) reported through the Quality and Performance Committee and the Trust Leadership Team.
The Trust has a Caldicott Guardian, a dedicated Board member who is responsible for protecting the confidentiality of people’s health and care information and making sure it is used properly. We also have a Senior Information Risk Owner (‘SIRO’), a dedicated Board member with responsibility for assuring the Board regarding information security and risks.
As part of the Trust’s responsibilities under the Data Protection Act (2018), we also have a dedicated Data Protection Officer who has responsibility for:
• Informing and advising on data protection laws
• Monitoring compliance with Privacy and data protection laws, data protection polices, including managing internal data protection activities, raising awareness of data protection issues, training staff and conducting internal audits
• Cooperating with the supervisory authority
• Being the first point of contact for supervisory authorities and for individuals whose data is processed (employees, users of our services, carers etc).
The Data Protection and Security Toolkit (DSPT) is the mandated method for monitoring the Trust performance in the key areas of data protection and technical/cyber security on an annual basis. For the 2023/2024 submission this is based on the NHS Data Security Standards and is focussed on ensuring the Trust remains compliant with laws concerning the handling and sharing of personal information, along with remaining resilient to cyber threats. The DSPT Standards for 2023/2024 required the Trust to submit 108 evidence items to support 34 mandatory assertions. The Trust achieved a ’Standards Met’ status.
The 2024/2025 DSPT submission sees a move away from measuring performance against the National Data Guardian’s 10 data security standards and instead adopts the National Cyber Security Centre’s Cyber Assessment Framework (CAF) as its basis for cyber security and IG assurance. The Trust is currently working towards 2024/2025 submission.
The Trust adheres to the guidance issued by NHS Digital: ‘Guide to the Notification of Data Security and Protection Incidents. All IG incidents are subject to a robust internal assessment and investigation process to understand the cause and consequences of the breach, the actions taken/required, and shortcomings identified and addressed. Where the incident is assessed as being reportable to the Information Commissioners Office as a serious incident then the Trust submits this through the Data Security and Protection Toolkit.
One incident was reported to the Department of Health and Social Care and ICO via the Data Security and Protection Toolkit during the period 1st April 2024 to 31st March 2025. This incident was fully investigated by the Trust and appropriate actions undertaken. The ICO considered the incident have informed the Trust that no further action would be taken by them. The ICO have made recommendations to minimise the risk of such incidents reoccurring, all recommendations are followed up with evidence to support completion. The table below provides detail of the incidents reported.
| Data breach incidents reported to DHoSC and ICO | |
|---|---|
| Reported to Supervisory body | Type of Breach - Summary - Outcome |
| 15/08/2024 | Confidentiality & Integrity Breach – Letter sent to patients home address, against the consent wishes of the patient and was accessed and read by patients husband. Incident closed by ICO; no further action taken by the ICO. |
The Trust is committed to ensuring compliance with statutory, legislative, and national frameworks/guidance to embed robust data security and information handling practices.
Data quality and governance
The Trust has a data quality improvement plan in place which is monitored through the contracting process with commissioners. The Trust audit plan includes a rolling programme of audit against performance and quality indicators.
2024/25 is the sixteenth year of publishing a Quality report for the Trust. The Trust has drawn upon service user, carer, and staff feedback as well as the Council of Governors to inform the Quality Account. We have also listened to stakeholder feedback on areas for improvement and our response to these are incorporated in the 2024/25 Quality Report. This engagement has also contributed to the development of our quality priorities for the year ahead.
The Trust set an overarching annual plan which included a range of service priorities and quality priorities for 2024/25. The service priorities have formed part of our key programmes of work during the year across inpatient services, urgent care, community services, children and young people and learning disabilities and autism.
As part of the national requirement to define a set of priorities as part of the Quality Account, priorities were identified for 2024/25:
•Quality Priority 1: Implement PSIRF (Patient Safety Incident Response Framework) – ongoing from 2023-24
•Quality Priority 2: Delivering on the key learning from safety improvement themes:
o Reduce Violence
o Improve Physical Healthcare
o Reduction in Suicides
o Reduce Restrictive Practice
• Quality Priority 3: Ensure that the six principles of the Triangle of Care are fully embedded throughout the organisation.
• Quality Priority 4: Embed learning through research and informing improvements in care delivery.
• Quality Priority 5: Embed a culture of Trauma Informed Care and its approaches across the organisation.
Reporting against delivery of these priorities has taken place throughout the year.
The Trust strategy ‘With You in Mind’ sets out five key strategic ambitions for the future. Our first ambition is to achieve quality of care, every day, which has formed the basis for the priorities we have set for 2024/25. These are:
• Implementation and embedding of PSIRF.
• Delivering on the learning from key safety improvement themes:
o Reduce violence
o Improve physical healthcare
o Reduction in suicides
o Reduce restrictive practice
• Ensure that the six principles of the triangle of care are fully embedded throughout the organisation.
• Embed learning through research and informing improvement in care delivery.
• Embed a culture of Trauma Informed Care and its approaches across the organisation.
The Chief Operating Officer has overall responsibility to lead the production and development of the Quality Account/report. A formal review process was established, the Quality Account drafts were formally reviewed through the Trust governance arrangements (Executive Directors, Quality and Performance Committee, Audit Committee, Council of Governors, and Board of Directors) as well as being shared with partners.
The Trust has put controls in place to ensure the accuracy of the data used in the Quality Account. These controls include adherence to the Trusts Data Quality Policy
Systems and processes have been further improved across the Trust during 2024/25 with the continued expansion of the near real-time dashboard reporting system. This reports quality indicators at every level in the Trust from patient/staff member to Trust level, including a review of options within system picklists to ensure data accuracy for reporting both national and local data.
The Trust has training programmes in place to ensure staff have the appropriate skills to record and report quality indicators. Key training includes:
• Electronic Patient Record (RiO)
• Trust Induction
• Data Security Awareness
The Trust audit plan includes a rolling programme of audits on quality reporting systems and metrics. The Internal Audit Plan is fully aligned to the Trust’s Board Assurance Framework and integrates with the work of clinical audit where this can provide more appropriate assurance.
Through the engagement and governance arrangements outlined above the Trust has been able to ensure data quality and the Quality Account/Report provides a balanced view of the organisation and appropriate controls are in place to ensure the accuracy of data. Data quality is also monitored through the monthly Integrated Performance Report highlighting data quality of measures using a RAG rating system.
Review of effectiveness
As Accounting Officer, I have responsibility for reviewing the effectiveness of the system of internal control. My review of the effectiveness of the system of internal control is informed by the work of the internal auditors, clinical audit and the executive managers and clinical leads within the Trust who have responsibility for the development and maintenance of the internal control framework. I have drawn on performance information available to me. My review is also informed by comments made by the external auditors in their management letter and other reports. I have been advised on the implications of the result of my review of the effectiveness of the system of internal control by the Board, the Audit Committee and Board Committees and a plan to address weaknesses and ensure continuous improvement of the system is in place.
The Trust’s governance framework provides me with assurance and evidence that the effectiveness of controls in place to manage the risks associated with achieving key organisational objectives have been systematically reviewed. Internally I receive assurance through the operation of the governance framework as described in this statement, including the Trust-wide Governance Structures, Board and Committee structures, operational/delivery structure, group level governance structures, internal audit reviews and the Audit Committee. I have received additional assurance throughout the 2024/25 year based on the substantial reviews undertaken associated with the Board Assurance framework and risk appetite, the Trust’s risk management processes and policy, and the governance framework.
My review is also informed by on-going registration inspections and Mental Health Act reviewer visits by the Care Quality Commission, External Audit activity, NHS England’s ongoing assessment of the Trust’s performance, the N NC Integrated Care Board’s provider oversight meetings, on-going review of performance and quality by our commissioners and self-assessment and internal audit of Trust’s leadership and governance against CQC Well Led Framework.
Throughout the year the Audit Committee has operated as the key standing Committee of the Board with the responsibility for assuring the Board that effective processes and systems are in place across the organisation to ensure effective internal control, governance, and risk management. The Audit Committee is made up of three Non-Executive Directors and reports directly to the Board. The Committee achieves its duties through:
• Overseeing the risk management system and obtaining assurances that there is an effective system operating across the Trust. Reviewing the establishment and maintenance of an effective system of integrated governance, risk management and internal control across the Trust that supports the achievement of the organisations objectives.
• Consideration of the systems and processes in place to maintain and update the Board Assurance Framework, and consideration of the effectiveness and completeness of assurances that documented controls are in place and functioning effectively.
• Scrutiny of the corporate governance documentation for the Trust.
• The agreement of external audit, internal audit and counter fraud plans and detailed scrutiny of progress reports. The Audit Committee pays particular attention to any aspects of limited assurance, any individual areas within reports where issues of risk have been highlighted by internal audit, and on follow up actions undertaken. Discussions take place with both sets of auditors and management as the basis for obtaining explanations and clarification.
• Receipt of assurance updates at meetings from Executive/Service Leads following Limited assurance reports being given.
• Receipt and detailed scrutiny of reports from the Trust’s management concerning the governance and performance management of the organisation, where this is considered appropriate.
• Review of its own effectiveness against national best practice on an annual basis. The terms of reference for the committee were adopted in line with the requirements of the Audit Committee Handbook and the NHS Code of Governance.
The Board itself has a comprehensive system of performance reporting. This includes analysis against the full range of performance and compliance standards, regular reviews of the Board Assurance Framework, ongoing assessment of clinical risk through complaints, serious incidents, incidents, lessons learned, as well as focusing the strategic, long-term issues for the organisation. The Quality and Performance Committee receives a regular update on the performance of clinical audit. The Audit Committee also dedicates specific time throughout the year to monitor and review areas of clinical risk, quality, and safety issues. The Audit Committee has also implemented a cycle of reporting from other Board Committees to receive further assurance on the management of risks and internal control.
There are several processes and assurances that contribute towards the system of internal control as described above. These are subject to continuous review and assessment. The systems, frameworks and processes described in this statement has identified no significant gaps in control and where gaps in assurance have been identified, actions are in place to ensure that these gaps are addressed.
Conclusion
My review confirms that Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust and the group has a generally sound system of internal control that supports the achievement of its policies, aims and objectives. No significant internal control issues have been identified.
James Duncan
Chief Executive
25 June 2025