Patient and Carer Race Equality Framework (PCREF)
This section explains some of the language and ideas we talk about in this report. It might be helpful to understand what we mean when we use these terms before reading the rest of the report.
Sex
The Equality Act 2010 is a law which protects people from unfair treatment. The law says your biological sex is either male or female, and that your sex is the one listed on your birth certificate. The biological sex listed on your birth certificate is usually based on your genitals at birth. This is not the only way to understand biological sex. Your reproductive organs, hormones, and chromosomes are also part of biological sex.
Some people might feel excluded by the legal definition of biological sex. For example, people who are intersex, trans, or have differences of sexual development.
Gender
Biological sex and gender identity are different things.
Gender identity is our internal feelings about being a man, woman, both or neither. Even though people might use the same word to describe their gender identity, we all have a unique experience of gender.
Gender identity can stay the same, or it can change. You might feel a different gender than the sex you were assigned at birth. If you choose to, you can apply to change your legal gender.
Sexuality
Sexuality and sexual orientation are about how people are attracted to other people. Some people feel emotional, physical or romantic attraction to others. Some people don’t experience these attractions.
Your sexuality is not linked to your biological sex or to your gender identity. You cannot know a person’s sexuality by knowing their biological sex or gender identity.
Research shows that lesbian, gay, bisexual, trans and other LGBTQ+ people experience unfair differences in health compared to heterosexual (straight) and cisgender people. (Cisgender means someone whose gender identity is the same as the sex recorded on their birth certificate).
You can find out more about language used to describe sex, gender and sexuality from the charity Stonewall.
Ethnicity
Ethnicity describes the population group a person belongs to or identifies with. What people consider part of their ethnic identity can be different for different people. It can include aspects like ancestry, culture, identity, religion, language, and appearance.
The Equality Act 2010 is a law which protects people from unfair treatment. This law says ethnicity includes skin colour, nationality, and ethnic or national origins. It protects people from unfair treatment because of these traits.
Ethnicity categories
The Office for National Statistics (ONS) produces information about the UK population. The ONS uses five main ethnicity categories. These categories are Asian, Black, Mixed, Other and White. We have used the same categories in this report.
Each of these contains smaller categories. These can describe people’s ethnicity in more detail:
- Asian. This includes Asian or Asian British, Pakistani, Indian, Bangladeshi or Other Asian background.
- Black. This includes Black or Black British, African, Caribbean, and Other Black background.
- Mixed. This includes White and Asian, White and Black African, White and Black Caribbean, and Other Mixed background.
- Other. This includes Chinese, Arab, and other ethnic groups.
- White. This includes White British, Irish, and Other White backgrounds including Gypsy and Roma.
Patient and Carer Race Equality Framework (PCREF)
NHS England is the organisation which runs the NHS in England. NHS England has asked all NHS trusts which provide mental health support to develop a plan to stop unfair treatment of people from minority ethnic and cultural groups. NHS organisations need to work together with local communities who experience unfair treatment to develop the plan. This plan is called the Patient and Carer Race Equality Framework (PCREF).
Find out more about the Patient and Carer Race Equality Framework.
Racialised and Culturally Minoritised Backgrounds
Some people think the language in laws and government documents doesn’t match their cultural identity and experience.
The Patient and Carer Race Equality Framework refers to "racialised and culturally minoritised communities." In this report, we also use this phrase. It includes
- Ethnic, racial, and cultural communities that are minoritised in England. These groups face marginalisation and have been racialised. This means society categorises them based on appearance and makes unfair judgments.
- People with different cultural or ethnic identities. This includes people who speak various languages and have diverse cultural traditions, as well as different spiritual or religious beliefs. White minorities include Gypsy, Roma and Irish Traveller groups and Jewish people.
Index of Multiple Deprivation
In England, we use the Index of Multiple Deprivation. It helps us see how many resources and services people have and if they live in safe, healthy environments.
This system gathers data on living conditions, income, jobs, education, health, crime, and access to housing and services. Each postcode area in England gets a score. This shows which areas have the worst access to resources and safe environments (most deprived) and which have the best (least deprived).
The Index splits all English postcode areas into five groups based on their score. Each group represents 20% of the population, from the most deprived to the least deprived. These groups are called ‘quintiles’. Knowing a postcode's quintile helps us understand how much access people in that area have to resources and services compared to others.
CNTW area
‘CNTW area’ means the areas where our Trust provides services. These are Northumberland, Newcastle, North Tyneside, North Cumbria, Gateshead, Sunderland, and South Tyneside.
Census 2021
The Census is a national survey. It is carried out by the Office for National Statistics every 10 years. The Census asks questions about the person filling out the survey, the people they live with, and where they live. Census data helps the government and local authorities plan and fund services in the community. This includes schools, doctors’ surgeries, and roads.
The last Census was held in 2021. We have used information from the 2021 Census in this report.
About Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust (CNTW)
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust (CNTW) is part of the NHS. We support people in North Cumbria, Northumberland, Newcastle, North Tyneside, Gateshead, South Tyneside, and Sunderland.
We specialise in mental health and learning disabilities. Our support covers people of all ages with various needs.
We employ around 9,000 staff and spend over £500 million each year on our services. We assist people in their homes, local communities, and hospitals.
This report focuses on unfair differences in our services. To reduce these differences, senior staff lead specific efforts to address health inequalities. This report does not describe all the work our organisation is doing to tackle health inequalities. Only the projects linked to the themes in this report are included. Our Trust Board will ensure we collaborate with communities, patients, and carers to tackle these unfair differences.
Our Vision
At CNTW we want to work together with compassion and care, to keep you well over the whole of your life. To achieve our aim, we must better understand and address health inequalities.
What are health inequalities?
Health inequalities are the gaps in health between different groups. These differences are unfair and can be avoided. For example:
- People who are poorer, live in unsafe or unhealthy places, or have trouble getting health services usually have shorter lives. In the North East and North Cumbria, people often die younger than in other parts of England.
- During the pandemic, non-White people in the UK were more likely to die from Covid-19 than White people. People from Pakistani and Bangladeshi backgrounds had the highest risk of dying from the virus.
Using Data to Understand Health Inequalities
Understanding health inequalities can be difficult. Often, there are many causes. We use ‘data’ to refer to the information we gather about our services and their users. In the NHS, we collect a lot of data. This helps us explore what might cause unfair health differences.
Data is a good starting point for understanding inequalities. But it doesn't provide all the answers about the causes of these unfair differences. We need to collaborate with local communities to see how these issues affect you and your health. It's important to understand how you feel about getting support from CNTW. We also need to hear from our communities about what changes we need to make. This ensures our services are welcoming and meet everyone’s needs.
About this report
This report provides a summary of data about some of the services CNTW provides:
- Talking Therapies
- Children and young people’s access to mental health services
It also includes a summary of data about what can happen to people when they need to be cared for in one of our hospitals:
- Being kept in hospital under the Mental Health Act
- Restrictive interventions
We explain these services and types of care in more detail later this report.
In this report we talk about unfair differences in health linked to age, ethnicity, biological sex, and deprivation. We also look at whether people have access to safe and healthy environments and the resources and services they need to stay well. In the next section of this report, we explain what we mean when we use these terms. We have included a more detailed explanation in the Glossary section at the beginning of this report.
We collected the data included in this report between April 2024 and March 2025.
This report uses past data from our electronic patient records and official statistics. It is experimental. The data may differ from official statistics published by NHS England or CNTW. The report might be incomplete if CNTW lacks information on a patient’s sex, age, ethnicity, or level of deprivation.
Key messages in this report
Health inequalities
- Health inequalities are the gaps in health between different groups. These differences are unfair and can be avoided.
Using data to understand health inequalities
- Data can be a helpful starting point for understanding inequalities. But it doesn’t tell us everything we need to know about what causes unfair differences in health. We need to listen to feedback from our communities about what needs to change.
Detentions under the Mental Health Act
- In the CNTW area, 86 people per 100,000 population were detained under the Mental Health Act between April 2024 and March 2025. This rate is lower than the previous year. In 2023/24, 91 people per 100,000 population were detained under the Mental Health Act.
- The rate of detentions is higher among younger people (18-45), and among people aged 76 and over.
- The detention rate for males was higher than for females in 2024/25. While the detention rate for males in CNTW in 2024/25 is similar to last year, the detention rate for females has reduced.
- The rate of Mental Health Act detentions is highest in more deprived areas.
- Compared to the previous year, detention rates for people from the most deprived areas have reduced. There has been a small increase in the detention rates for people from less deprived areas.
Restrictive Interventions
- On average, from April 2024 to March 2025, CNTW patients faced restrictive interventions 48 times for every 1,000 hospital days.
- The rate of restrictive interventions has gone up compared to last year. In 2023/24, patients faced restrictive interventions 41 times for every 1,000 hospital days.
- The rate of restrictive interventions is higher in the younger age groups and is highest among people aged 17 and under.
- Female patients experience a higher rate of restrictive interventions.
- The rate of restrictive interventions is highest for patients with a Mixed ethnicity.
- The rate of restrictive interventions for patients from different ethnic groups has changed since 2023/24.
Talking Therapies recovery
- The overall Talking Therapies recovery rate for our Trust is 53%.
- Since 2023/24, recovery rates have risen the most for the youngest (under 26) and oldest (over 76) age groups.
- Talking Therapies recovery rates are similar for male and female patients.
- In 2024/25 Asian patients had the highest Talking Therapies recovery rate at 63%.
- Patients with an ethnicity categorised as Other had the lowest recovery rate at 32%.
- People living in more deprived areas have lower recovery rates. This is the same as the previous year. But there have been small increases in Talking Therapies recovery rates in the most deprived groups.
Access to Children and Young People’s Services
- Older children have a higher rate of contact with CNTW services than younger ones. In 2024/25, more children and young people aged 6 to 13 had contact with CNTW services than in the previous year.
- More boys than girls have had at least one contact with CNTW services.
- Most children and young people who were in contact with CNTW services from April 2024 to March 2025 were White (92%).
- Children and young people in the most deprived areas have the highest rate of contact with our services.
Detentions under the Mental Health Act
The Mental Health Act is a law which says when you can be taken to hospital, kept there, and treated against your wishes. This should only happen if you have mental health issues that put you or others at risk, and there are no other ways to keep everyone safe.
Being in hospital or ‘detained’ under the Mental Health Act is often called being ‘sectioned’. This term comes from the law’s different sections. Some parts of the Mental Health Act help treat people with mental illness involved in the criminal justice system. If you are on remand in prison and have a serious mental illness, you can be moved to a mental health hospital. The data presented in this report covers detentions under all sections of the Mental Health Act.
This year, we will deliver projects to lower the number of people from marginalised ethnic backgrounds admitted to our hospitals under the Mental Health Act. We will partner with local community groups, patients, and carers from marginalised ethnic, cultural, and faith backgrounds. This is part of our effort to improve services for these groups. We will use what we learn from these projects to address other unfair differences in how the Mental Health Act is applied.
Number of detentions
- 1,522 people were detained under the Mental Health Act in the CNTW area between April 2024 and March 2025. In 2024/25 there were 87 fewer detentions than in the previous year.
- 150 people were detained in CNTW who are registered with a GP outside the CNTW area. This might happen because:
- The person being detained is cared for by a CNTW service which accepts patients from the whole of the North East or the whole of England.
- If there are no mental health hospital beds near a person’s home, they go to a CNTW hospital instead.
- Someone is away from home or doesn’t have a stable home, and are in the CNTW area when they need to be detained.
Rate of detentions per 100,000 population
We use a rate per 100,000 population to understand differences in the use of Mental Health Act detentions between different groups. This rate describes how many times the Mental Health Act is used to take someone to hospital, keep them there, and treat them against their wishes for every 100,000 people.
Using a rate of detentions per 100,000 people helps us see if there are unfair differences in how the Mental Health Act is used across different groups in society. This works even if one group has many more people than another, which could lead to big differences in the actual number of detentions.
- In the CNTW area, 86 people per 100,000 population were detained under the Mental Health Act between April 2024 and March 2025.
- This overall detention rate is lower than the previous year. In 2023/24, 91 people per 100,000 population were detained under the Mental Health Act.
Age
The chart below shows how the number of detentions per 100,000 population varies with age.
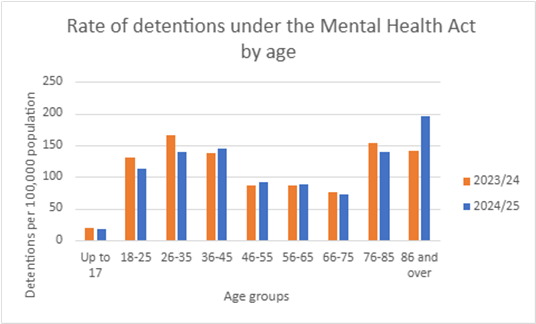
The rate is higher among younger people (18-45), and among people aged 76 and over. This pattern in detention rates is similar to the previous year. But rates have decreased in the under 36 age groups and increased in the 86 and over age group. In 2024/25 the 86 and over age group had the highest rate of detention under the Mental Health Act. In the previous year the 26-35 age group had the highest rate of detention.
Evidence shows that people are more likely to first experience psychosis (seeing and hearing things other people don’t) in their late teens and early 20s. A person might need to be detained under the Mental Health Act if their symptoms of psychosis put them or someone else at risk of harm.
More people with dementia and older adults facing mental health issues are also being detained under the Mental Health Act. Our Trust cares for a lot of patients with dementia. This could explain why we see higher rates of detention among older people.
Sex
There are some differences between the detention rates for males and females:
- 101 detentions per 100,000 males
- 86 detentions per 100,000 females
The detention rate for males was higher than for females in CNTW in both 2024/25 and in the previous year. National Mental Health Act data shows that males in England have a higher detention rate over several years. While the detention rate for males in CNTW in 2024/25 is similar to last year, the detention rate for females has reduced.
We have more beds for male patients than for female patients. This means we are able to provide care to more males than females detained under the Mental Health Act in our hospitals. This may explain, at least partly, why the detention rate is higher for males in our Trust. We also need to think about whether the difference in detention rates is linked to varying access to social support networks and community mental health support.
Deprivation
The chart below shows the rate of Mental Health Act detentions in our communities. They are grouped by deprivation level. The rate of Mental Health Act detentions is highest in more deprived areas. This is also the case in England as a whole.
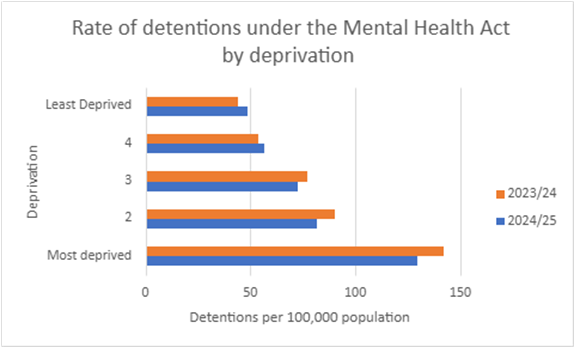
Compared to the previous year, detention rates for people from the most deprived areas have reduced. There has been a small increase in the detention rates for people from less deprived areas.
Ethnicity
The table below lists how many times people from each ethnic group were admitted to our hospitals under the Mental Health Act in 2024-25:
| Ethnicity | Asian | Black | Mixed | Other | White |
|---|---|---|---|---|---|
| Admissions under the Mental Health Act | 62 | 53 | 20 | 24 | 1,443 |
We won’t include a rate of Mental Health Act detentions by ethnic groups in this year’s report. We aren't sure we have accurate information on the size of different ethnic groups in our Trust area. To see if there are unfair differences in how the Mental Health Act is used with different ethnic groups, we need to calculate the detention rate for each group. We can’t do this using the data we record about the number of detentions. One ethnic group might contain a lot more people than another group. This would result in big differences in the actual number of detentions. We need to know the size of each ethnic group. This helps us calculate the detention rate for each group accurately. Then, we can compare the rates between different groups. This is the only way to see if people from different ethnic groups are more likely to be detained under the Mental Health Act.
Detention rates for each ethnic group usually come from the 2021 Census data on ethnicity. We compared the 2021 Census data with other information about people’s nationality and ethnicity. This included adults of various nationalities registering for National Insurance numbers in the CNTW area. It also covered the number of children from different ethnic backgrounds in our local schools. There were some big differences. Community leaders from minoritised backgrounds in our Trust area told us their communities have grown a lot in recent years. Detention rates based on ethnicity data from the 2021 Census may be wrong. This is why we have decided not to include detention rates for different ethnic groups in this report.
Use of restrictive interventions
Restrictive interventions are actions that limit someone’s movement or freedom. These actions are used to reduce the risk of danger to a person or the people around them. They include:
- Seclusion – patients are kept in an area away from other patients. They are not able to leave that area and are supervised by hospital staff.
- Long-term segregation - patients cannot mix freely with others on the hospital ward for an extended time.
- Manual restraint – physically holding a person’s body to limit their movement.
- Mechanical restraint – using handcuffs or other equipment to limit someone’s movement.
- Chemical restraint – using medication which is not prescribed as part of the patient’s usual care. This might include rapid tranquillisation.
- Blanket restrictions – rules applied to all patients on the ward which restrict their movement or freedom. For example, searching all patients when they come back to the ward if there’s evidence illegal drugs have been brought in to the unit.
Mental health hospitals care for people who are very unwell. They help those with severe symptoms that make community care unsafe. In hospital, situations can develop which put patients and staff at risk of harm. Hospital staff must take action to reduce the risk and keep everyone safe. Sometimes, we need restrictive interventions to lower the risk of harm. They should only be used when a situation can’t be made safe without limiting someone’s movement or freedom.
Our staff often guide our patients' behaviours and decisions in a supportive way. This can sometimes limit their freedom or movement. Our staff also help patients with personal care, like getting ready, washing, and using the toilet, whenever needed. Our staff are aware of the need to keep a record of care which limits a patient’s freedom or movement. Our data on restrictive interventions will likely cover these care types. It will also include more restrictive methods, such as seclusion or rapid tranquillisation.
NHS Trusts, including CNTW, are working to cut down on restrictive interventions in our care. We’ve gained a better understanding of why, when, and how we use restrictive interventions. This will help us address unfair differences in using restrictive interventions in 2025/26. In the next year, we will focus on ethnicity in our Trust's efforts to reduce restrictive interventions. This is a key objective of our plan to tackle inequalities in our services linked to ethnicity, faith and culture.
Rate of restrictive interventions per 1,000 days spent in hospital
We measure the 'rate of restrictive interventions per 1,000 hospital days' to see how different groups receive care that limits movement or freedoms.
When we say ‘rate of restrictive interventions per 1,000 days in hospital’, we mean how often someone has their movement or freedom limited for every 1,000 days people from that group spend in hospital.
Using the this rate instead of the total number of restrictive interventions helps us understand whether there are unfair differences in how this type of care is used between different groups.
Not all patients have their freedom or movement limited when they are in hospital. Some patients may need stricter interventions than others, depending on the situation, to keep everyone safe. These differences between individual patients can have a big impact on the rate of interventions for particular groups, and CNTW patients overall.
- CNTW used care which limited the movement or freedom of our patients 10,473 times between April 2024 and March 2025.
- During the same period, our patients spent a total of 219,819 days in hospital.
- On average, CNTW patients experienced restrictive interventions 48 times for every 1,000 days spent in hospital.
- The rate of restrictive interventions has gone up compared to last year. In 2023/24, patients faced restrictive interventions 41 times for every 1,000 hospital days.
Age
The chart below displays the rate of restrictive interventions for every 1,000 hospital days, broken down by age group. The rate of restrictive interventions is higher in the younger age groups.
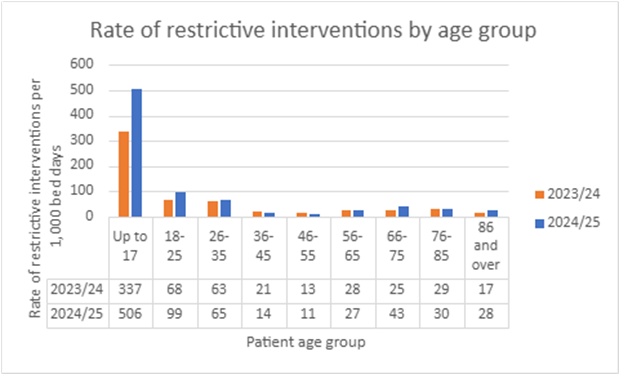
The rate of restrictive interventions is highest for those aged 17 and under. It stands at 506 interventions for every 1,000 days in hospital. This is a big increase from the previous year. In 2023/24, there were 337 restrictive interventions for every 1,000 days spent in hospital for those aged 17 and under. In 2024/25, the rate of restrictive interventions rose significantly for those aged 18-25, 66-75, and 86 and over.
Senior members of staff from our Trust are leading a review of the care we provide to children and young people. We want to better understand how, when and why we limit the freedom or movement of young people in our care, and what we can do to reduce it.
Sex
There is quite a big difference between males and females in the use of care which limits people’s movements or freedom:
- 58 restrictive interventions per 1,000 days spent in hospital for females.
- 41 restrictive interventions per 1,000 days spent in hospital for males.
We think this could be because female patients are more likely to try to hurt themselves while they are in hospital. In these situations, it is very risky not to take action to keep the patient safe.
Ethnicity
There are differences between ethnic groups in the use of care which limits people’s movement or freedom. The chart below shows the rate of restrictive interventions for each of the five main ethnic groups in 2024/25.
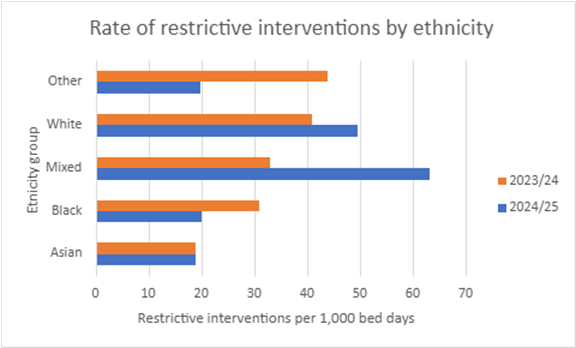
When we compare these rates to the previous year, we see some big differences:
- The rate of restrictive interventions for Asian patients was 19 per 1,000 hospital days in both 2023/24 and 2024/25.
- There was a large decrease in the rate of restrictive interventions for Black patients. This dropped from 31 restrictive interventions per 1,000 hospital days in 2023/24 to 20 per 1,000 days in 2024/25.
- The rate of restrictive interventions for patients with a Mixed ethnicity almost doubled. It went from 33 restrictive interventions per 1,000 days spent in hospital during 2023/24 to 63 per 1,000 days spent in hospital in 2024/25.
- The rate of restrictive interventions for White patients rose from 41 per 1,000 hospital days in 2023/24 to 50 in 2024/25.
- The rate of restrictive interventions for patients in the Other ethnicity category dropped by over 50%. It went from 44 restrictive interventions per 1,000 days spent in hospital during 2023/24 to 20 per 1,000 days spent in hospital in 2024/25.
The number of restrictive interventions received by individual patients can have a big impact on the rate of interventions for particular groups of patients. If a few patients from one ethnic group have many restrictive interventions, the rate for that group can rise significantly that year. This may, in part, explain why we see big differences in the rate of restrictive interventions from year to year.
Deprivation
The chart below displays the rates of restrictive interventions for every 1,000 days in hospital for people in areas with different levels of deprivation.
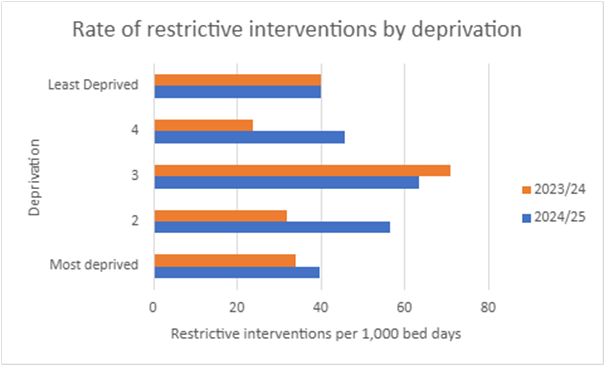
The highest rate is for those in the third segment, or ‘quintile,’ who don’t live in our most deprived or privileged communities. This was also the case in the previous year. But the rate of restrictive interventions for this group has dropped, from 71 per 1,000 hospital days in 2023/24 to 63 per 1,000 days in 2024/25.
The rate of restrictive interventions for people in the most deprived areas has gone up since last year. There was a large increase for people in the second most deprived area (quintile 2). It rose from 32 restrictive interventions per 1,000 days spent in hospital during 2023/24 to 56 per 1,000 days spent in hospital in 2024/25. The rate of restrictive interventions rose by nearly 50% for people in the second least deprived area (quintile 4). It went from 24 restrictive interventions per 1,000 days spent in hospital during 2023/24 to 46 per 1,000 days spent in hospital in 2024/25.
Talking Therapies recovery
NHS Talking Therapies supports people with anxiety and depression. People work with their therapist to understand their problems, overcome their challenges, and achieve their goals. This involves talking with a therapist and doing practical exercises.
We provide Talking Therapies in Sunderland and North Cumbria. Talking Therapies are available across the CNTW area. But in Newcastle, Gateshead, South Tyneside, North Tyneside and Northumberland, the Talking Therapies service is not provided by CNTW.
When people are sent to Talking Therapies, they are assessed. This checks if their anxiety or depression symptoms are severe enough for a clinical diagnosis. A person is seen as 'recovered' after treatment if they met the clinical diagnosis criteria when referred but no longer meet them by the end of treatment.
Many people not seen as 'recovered' still feel their mental health has improved with help from Talking Therapies. And 'recovery' doesn't mean that patients stop facing challenges with their mental health. Recovery from mental health challenges can be a long and difficult journey. But Talking Therapies can help people manage their symptoms.
We use the term ‘Talking Therapies recovery rate’ to understand differences in recovery between different groups. We mean the percentage of all the people from that group who did not have symptoms of anxiety disorder and depression severe enough to meet the criteria for a diagnosis at the time they finished their Talking Therapies treatment.
5,603 patients in Sunderland and North Cumbria completed Talking Therapies treatment between April 2024 and March 2025. 53% of these patients were considered to have 'recovered'. The information in this section of the report is about these patients.
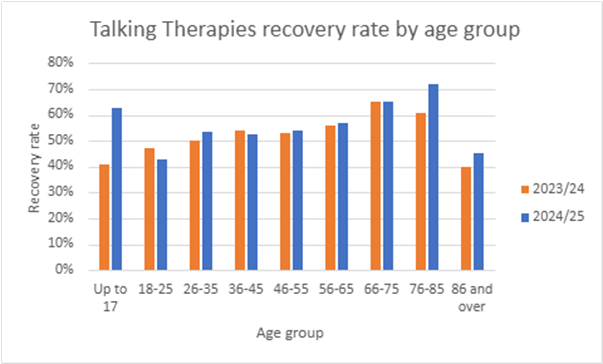
Age
The chart below shows the Talking Therapies recovery rate for different age groups. Since 2023/24, recovery rates have risen the most for the youngest (under 26) and oldest (over 76) age groups. At 53%, the overall Talking Therapies recovery rate is similar to the previous year, when it was 52%.
Sex
Talking Therapies recovery rates are very similar for male and female patients:
- 3% recovery for male patients (including trans men)
- 8% recovery for female patients (including trans women)
The recovery rate for male patients is up from last year’s 51%. The recovery rate for female patients is now slightly lower than last year's rate of 53%.
We use a different computer system to track information about patients in our Talking Therapies service. This enables us to collect data about Talking Therapies recovery for patients who identify as transgender or non-binary (people who don’t identify as either a man or woman). We can't share details about very small patient groups. This is because it might let someone identify individuals. People’s healthcare information must be kept private. Because of this, we haven’t included the Talking Therapies recovery rate for people who identify as non-binary in this report. Some of our Talking Therapies staff have completed training on gender and trans issues. They work closely with partners to make sure that the service meets the needs of people with different gender identities.
Ethnicity
The chart below shows the recovery rate for people from different ethnic groups who completed Talking Therapies in Sunderland and North Cumbria between April 2024 and March 2025.
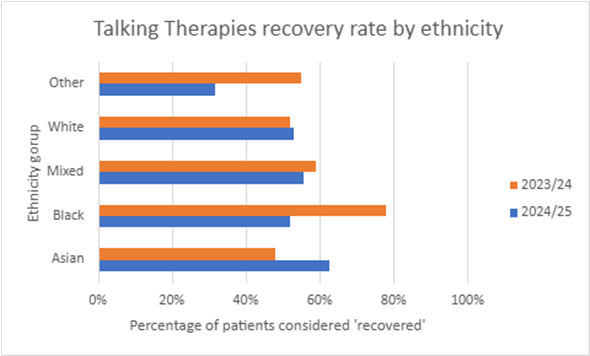
Compared to the previous year:
- The recovery rate for Asian patients increased from 48% to 63%.
- The recovery rate for Black patients reduced from 78% to 52%.
- The recovery rate for patients of mixed ethnicity dropped a bit, from 59% to 56%.
- The recovery rate for White patients increased slightly from 52% to 53%.
- The recovery rate for patients in the Other ethnicity category dropped from 55% to 32%.
The number of patients from each ethnic group who complete Talking Therapies can have a big impact on the recovery rate. A small number of patients from one ethnic group may complete Talking Therapies each year. This could partly explain the large differences in recovery rates for that group from year to year. Fewer people from marginalised ethnic backgrounds complete Talking Therapies than White people. We lack enough data to know if people from these communities have a better or worse experience with Talking Therapies compared to White people.
The NHS Race and Health Observatory is a team of experts. They focus on unfair health differences among people from racialised and culturally minoritised backgrounds. Their research shows that, in general, people from Black and ethnic minority communities have worse NHS Talking Therapies recovery rates than White people. (NHS Race and Health Observatory, ‘Ethnic Inequalities in Improving Access to Psychological Therapies (IAPT)’, November 2023). They also have less access to Talking Therapies than White people. People from Pakistani, Bangladeshi, Other Asian, Mixed White, Black Caribbean, and Other ethnic groups had worse recovery rates than those from other minoritised groups.
Research suggests that unfair differences in recovery rates for Talking Therapies come from:
- People from minoritised communities being more unwell when they first go to Talking Therapies.
- People from minoritised communities often live in areas with poorer access to resources, services, and safe, healthy environments.
- People from minoritised communities face longer waits for their first Talking Therapies appointment and for follow-up sessions.
Some of our Talking Therapies teams have trained to support people from various cultural backgrounds. When our Talking Therapies teams assess a patient, they ask about their ethnic and cultural background and any specific needs.
Deprivation
The chart below shows how Talking Therapies recovery rates vary by area.
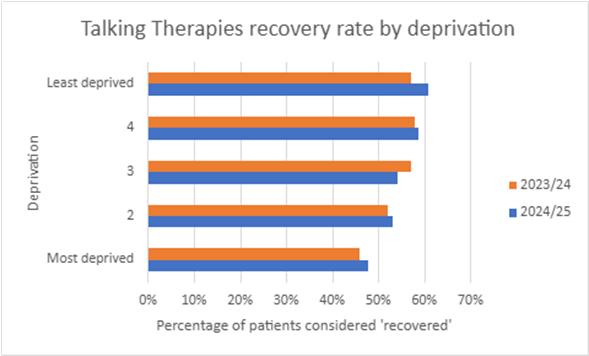
People living in more deprived areas have lower recovery rates. This is the same as the previous year. But, there have been small increases in Talking Therapies recovery rates in the most deprived groups. The largest rise in recovery rates from last year was in the least deprived group.
Living in a more deprived area could reduce the benefit people get from therapy and make recovery more difficult. Talking Therapies can support people to manage their mental health symptoms. But it can’t fix all the issues which might cause those symptoms like money worries, job insecurity, or poor quality housing. (Nuffield Trust, NHS Talking Therapies (IAPT) programme, updated April 2024).
Some of our Talking Therapies services offer Employment Advisers. These staff focus on helping people find a job or find a better job and stay in work. This can make a big difference helping people to improve their mental health.
Children and young people’s access to mental health services
This section is about children and young people’s access to mental health services. People have different ideas about what the term 'access' means. When we say 'access', we mean a young person aged 0 – 17 (up to and including the day before their 18th birthday) has had at least one contact with CNTW services. A 'contact' can mean a face-to-face appointment, a video call or a phone call. We include contact with the parent or carer of a child or young person, and conversations between staff involved in caring for a child or young person, in this definition. Emails and texts don’t count as contacts.
Senior staff in our organisation are leading a project on this topic. The aim is to understand and tackle barriers that prevent children and young people from different backgrounds from accessing our services. The project will focus on improving access to our services for children and young people from the least advantaged backgrounds and marginalised groups. We will work with children and young people and their families. We'll also work with local community organisations which support and represent children from different backgrounds.
Age
The chart below shows the number of children and young people per 1,000 who had at least one contact with CNTW services from April 2024 to March 2025.
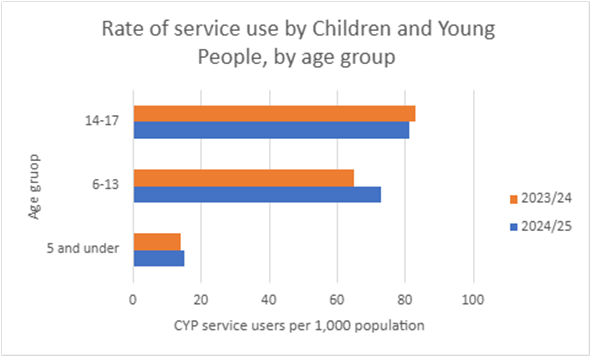
Older children and young people are more likely to receive at least one contact with CNTW services:
- 81 out of every 1,000 children and young people aged 14 to 17 had at least one contact with CNTW services from April 2024 to March 2025.
- In 2024/25, 73 out of every 1,000 children and young people aged 6 to 13 had at least one contact with CNTW services. This is an increase from the previous year. In 2023/24, 65 in every 1,000 children aged between 6 and 13 had at least one contact with CNTW services.
- 15 in every 1,000 children aged 5 and under had at least one contact with CNTW services in 2024/25.
Half of all mental health issues begin by the age of 14. Three quarters of mental health problems begin by the age of 24. (NHS England, NHS Long Term Plan, 2019). This could explain the higher contact rate with CNTW services for older children and young people. We need to work with our patients, communities, and partners. This will help us understand the differences better. Then, we can decide what actions to take to tackle any inequalities.
Sex
There is a difference in the rates that males and female children and young people access our services:
- 52 out of every 1,000 girls and young women in our area had at least one contact with CNTW services from April 2023 to March 2024.
- 61 out of every 1,000 boys and young men in our area had at least one contact with CNTW services.
Compared to the previous year, there was an increase in access rates for both male and female children and young people. There was a slightly bigger increase in the access rates for males. Research shows that in England, about the same number of boys and girls aged 8 to 16 face mental health issues. (NHS England, Mental Health of Children and Young People in England, 2023 – wave 4 follow up to the 2017 survey, November 2023).
Ethnicity
The table below shows the number of children and young people from various ethnic backgrounds who received at least one contact from CNTW mental health services:
This data alone doesn’t give us the full picture. We need more information to see if children and young people face unfair differences in access to mental health services based on ethnicity.
| Ethnicity | Asian | Black | Mixed | White | Other |
|---|---|---|---|---|---|
| Number of children and young people receiving at least one contact with CNTW services | 308 | 134 | 932 | 17,533 | 157 |
| % of patients | 2% | 1% | 5% | 92% | 1% |
Data from the 2021 Census shows big age differences between ethnic groups in England and Wales. The Census revealed that 18.5% of people in England and Wales were aged 0–15. In contrast, nearly half (48.6%) of those identifying as Mixed ethnicity White and Black African fell into the same age group. (Office for National Statistics ‘Ethnic group by age and sex, England and Wales: Census 2021’, January 2023).
To find out if there are unfair differences in access to mental health services for children and young people based on ethnicity, we need to know how many under-18s from each ethnic group live in the CNTW area. This would help us see if the differences in the number of children and young people from each ethnic group who contacted our services are due to the size of each group. Or, are these differences unfair and linked to inequalities we can address?
The number of children and young people from each ethnic group living in the CNTW area might have varied a lot since the 2021 Census. We’ve created a new way to understand how children and young people from marginalised ethnic backgrounds access our services. This is part of our work to tackle inequalities in our services linked to ethnicity, faith and culture. We will use this data to guide and track our plans. Our goal is to improve access to community mental health services for children and young people from marginalised ethnic backgrounds. These will be delivered in partnership with local communities.
Deprivation
The chart below shows the number of children and young people per 1,000 who received at least one contact from CNTW mental health services from April 2024 to March 2025 in various areas.
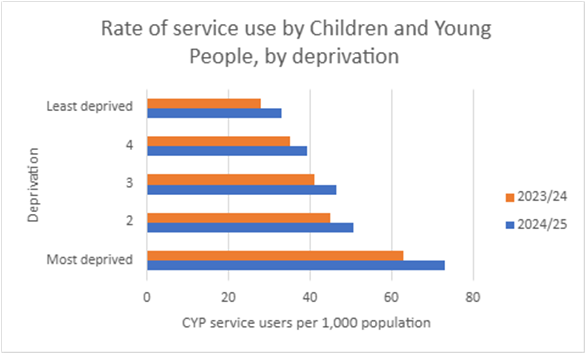
Using a rate per 1,000 people helps us see if there are unfair gaps in children and young people's access to mental health services across different areas. (When one area contains a lot more people than another, it can result in big differences in the actual number of children and young people accessing services.)
Children and young people in the most deprived areas have the highest rate of contact with CNTW services.
- In the most deprived areas, 73 out of every 1,000 children used CNTW services from April 2023 to March 2024.
- In the least deprived areas, 33 in every 1,000 children accessed CNTW services.
This is a similar pattern to last year. But in 2024/25, more children and young people accessed our services. This increase happened across all groups, from the most to the least deprived. The biggest increase in access rates was among children and young people from the most deprived areas. Children, young people, and their families in deprived areas may face tougher circumstances that threaten their mental health. This may result in more children and young people facing complex mental health issues. They might need more support from our services.
This report is available on request in other formats. We will do our best to provide a version of this report in a format that meets your needs. For other versions call 0191 246 6877, or email us at communications