Together: Service User and Carer Involvement Strategy
We believe that excellent care means treating people as whole humans and recognising that their mental and physical health are closely tied to each other. We know that many of the people in our care with a serious mental illness or learning disability and/or autism are at risk of dying over 20 years younger than their peers. Often these early deaths are due to physical illnesses that could have been prevented.
In this strategy we set out our ambitious goals to support those we look after to become and remain physically healthy as well as mentally healthy. Our aims below have grown from our conversations with service users and carers as well as our staff and partners in the wider healthcare system. It also reflects the commitments we have made in our Trust Wide strategy With you in mind. We believe physical health is everyone’s business, and that everyone has a part to play as part of our ‘Making Every Contact Count’ approach. We also believe that prevention is better than cure.
We want to ensure our service users remains physically healthy by:
- Using the tools already at our disposal to identify and treat physical health problems early on.
- Continuing to work closely with our service users and their carers and families to ensure our care is meeting their needs.
- Ensuring our staff are equipped with the knowledge and skills to support service.
- users with their physical health and any long-term physical health conditions.
- Looking closely at our inpatient and community environments to think about how we can best use these to support physical health.
- Working with our partners across the whole healthcare system to provide joined up care that recognises the importance of ensuring both physical and mental health simultaneously.
We have given careful thought to what we want to achieve and are delighted to note that our priorities echo many of those within the recently published 10 Year Health Plan for England, including a strong focus on prevention. Furthermore, we want to treat this strategy not as a final product but as a living and breathing reality.
For it to be useful and impactful it needs to be able to work with the challenges our teams face and the resources they have as those things change, all the while staying true to our core aim: ensuring everyone under our care has the support they need to live long lives free of the impact of physical illness, no matter who they are.

Sarah Glacken
Executive Director of Nursing, Therapies & Quality Assurance
Executive Summary
Our service users are living in poorer health and dying up to 20 years younger than their peers, often for unfair and avoidable reasons. A significant cause of early death and disability in our service users is poor physical health. This includes conditions such as heart disease, respiratory disease and cancer.
People with a serious mental illness or learning disability are also at an increased risk of poor outcomes in social metrics than can impact their physical health, such as access to stable employment, suitable housing and social support. They are more likely to have health damaging behaviours such as smoking, and are less likely to access screening programmes, which are a key part of identifying and treating physical health problems early. Unfortunately, they are more likely to experience ‘diagnostic overshadowing’ (where symptoms of a physical health problem are attributed to their mental health) which can result in significant delays in diagnosis and treatment. They can also suffer from poor physical health as a result of medication they take for their mental health problem.
All of this shows us clearly that physical health and mental health influence each other, and that support with physical health is both a key part of preventing mental illness and a core part of any mental health treatment offer. As a result, we have developed a strategy aimed at CNTW staff and professional partners that outlines how we will enable our service users to become and remain physically healthy.
Our strategy is founded on what physical health data tells us is needed, and what staff and service users told us were their main priorities across several listening events and our first ever Physical Health Summit. Prevention and a community-focused approach are also at the heart of our priorities, recognising that we can keep people well by providing them with the support, environment and access to services needed to prevent physical ill-health and to identify and address any physical health issues early.
Our aims to improve the physical health of those in our care also align with our wider trust ambitions:

Quality care, every day
We are dedicated to holistic, person-centred care that fully integrates physical and public health within mental health, learning disabilities, neuro disabilities and autism services. We will achieve this by supporting service users to engage with health promotion initiatives, recognising when physical health needs require prompt escalation, developing robust pathways for physical health liaison for service users in hospital and the community and rationalising medication use where appropriate.

Person-led care, when and where it is needed
We are committed to delivering service user-centred care that respects and celebrates the individuality of each person. We will achieve this by involving service users, family members and caregivers in decisions around care, identifying and addressing barriers that limit access to community care such as transport or language barriers, ensuring clear and accessible pathways for managing physical health conditions and improving the use of reasonable adjustment tools such as hospital passports.

A great place to work
We aim to prioritise staff well-being, empowering our teams to model and promote healthy behaviours and ensure staff are trained and equipped to address physical, public and mental health needs. We will achieve this by providing core physical health training from a trauma-informed perspective, developing shared training opportunities, supporting a health work environment for staff and supporting staff to become Physical Health Champions.

Sustainable for the long term, innovating every day
We strive to be flexible and innovative in addressing ongoing challenges to physical health within our communities, while ensuring successful practices remain sustainable. We will achieve this by using the buildings and grounds available to us to encourage physical activity, utilising technology to increase awareness of physical health support in the community and making environmental sustainability a key aspect of how physical health initiatives are assessed.

Working with and for our communities
We are committed to working with communities across the Trust (including service users, carers and staff) to ensure that services accurately reflect their needs and that everyone can access the support they need, regardless of where they live. We will achieve this by working in partnership with primary and secondary care and key organisations in the community, by developing a consistent physical health offer that has parity with our mental health offer and influencing commissioning processes to reflect impact on physical health.
Our service users are living in poorer health and dying up to 20 years younger than their peers often for unfair and avoidable reasons. A significant cause of early death and disability in our service users is poor physical health.
It is estimated that for people with a Serious Mental Illness (SMI*) 2 in 3 deaths are from physical illnesses that can be prevented2 while a 2022 report found that the top three causes of ‘avoidable deaths’ (defined according to the OECD/Eurostat lists of preventable and treatable causes of death for all people less than 75 years old) in adults with learning disabilities are heart disease, respiratory disease and cancer.3
This strategy sets out our vision for a service that enables the people in our care to become and remain physically healthy. It is underpinned by an understanding that physical health and mental health both influence each other, and that support with physical health is both a key part of preventing mental illness and a core part of any mental health treatment offer. The intended audience of this strategy includes CNTW staff and our professional partners in other parts of the health system and the community.
The purpose of this strategy is to provide clear direction to our staff and partners. It
outlines the key areas we need to address to ensure that our service users:
- have improved physical health outcomes
- understand the support offer for their physical health in the wider system
To identify the key areas of focus and improvement, we undertook several listening
events which consulted with our staff and service users to understand what
is important to the individual and ensure physical health becomes everyone’s business. The views expressed formed a core part of the priorities and aims set out in the following pages.
*As a strategy this document sets out our direction of travel and where we aim to get to. How these aims will be achieved will look different in every team as it would be impossible to capture the strengths and constraints of every team across our geography within one document. However, we have begun to develop a framework that outlines the key ways in which we can measure progress. This will be distributed internally and will support teams in drafting their implementation plans.
Our vision
To work and engage with service users in mind, to provide a holistic and collaborative approach to improve their physical and mental health. We will strive to remove health inequalities, Making Every Contact Count (MECC) and ensuring physical health is everyone’s business.

CNTW: Our people and places
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust is an organisation which employs almost 10,000 staff across our region and provides mental health, learning disability and rehabilitation support.
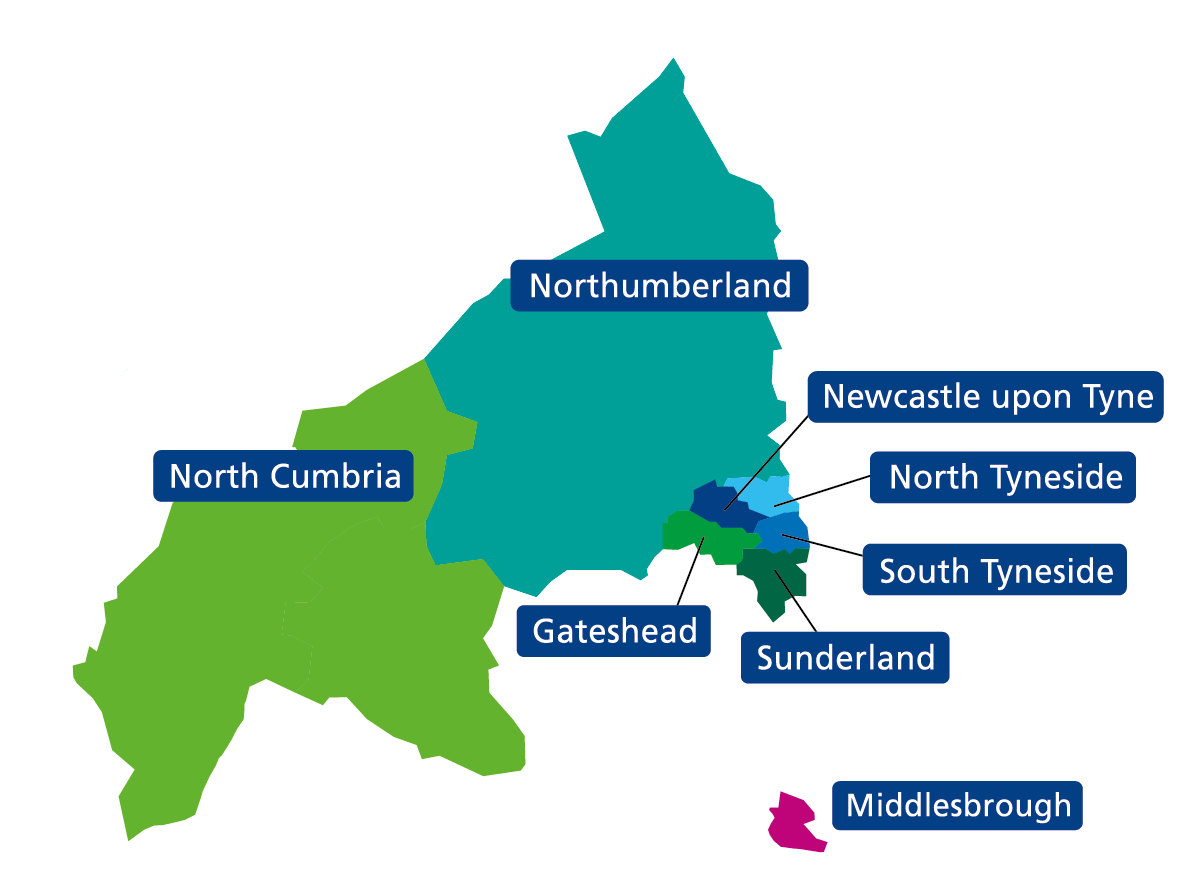
We spend more than £500 million each year, providing healthcare across North Cumbria, Northumberland, Newcastle, North Tyneside, Gateshead, South Tyneside and Sunderland.
Along with partners, we support people in their own homes, in their communities and in our hospitals. We provide support for people with long term complex needs and for those who require urgent or crisis care. We help:
- People with mental ill-health, including people with serious mental illness
- Children and young people
- People with a learning disability
- People with neurodevelopmental conditions
- People who need support from secure services
- People with neurodisabilities
- People with problematic substance use or addictive behaviours
We also provide specialist support such as perinatal mental health, mental health for deaf people and gender dysphoria services.
CNTW services are organised into three care groups – Community, Inpatient and Specialist. Our Specialist services include secure care services, children and young people’s (CYP) services, and services for people with neurodevelopmental conditions, neurodisabilities, learning disabilities and/or autism.
The diagram below shows the significant geographical area covered by CNTW. Our patch includes both highly compact urban areas (such as Newcastle and Gateshead) as well as widely dispersed rural areas (such as Northumberland and North Cumbria). Both contain communities that experience significant levels of deprivation, but the challenges
that deprivation causes in urban areas versus rural ones are different and require different solutions.
Our inpatient services form only the ‘thin part of the wedge’ of what we deliver, as seen below. The majority of our service users are cared for in their community, outside of our hospital sites.
A greater focus on community support allows people to access services in the places where they live and work, allowing them to integrate their care into the rest of their lives.
Our focus on community care and preventative actions recognises the importance of preventing ill-health in the first place, ensuring that people have the support and advice they need early on before they become more unwell.
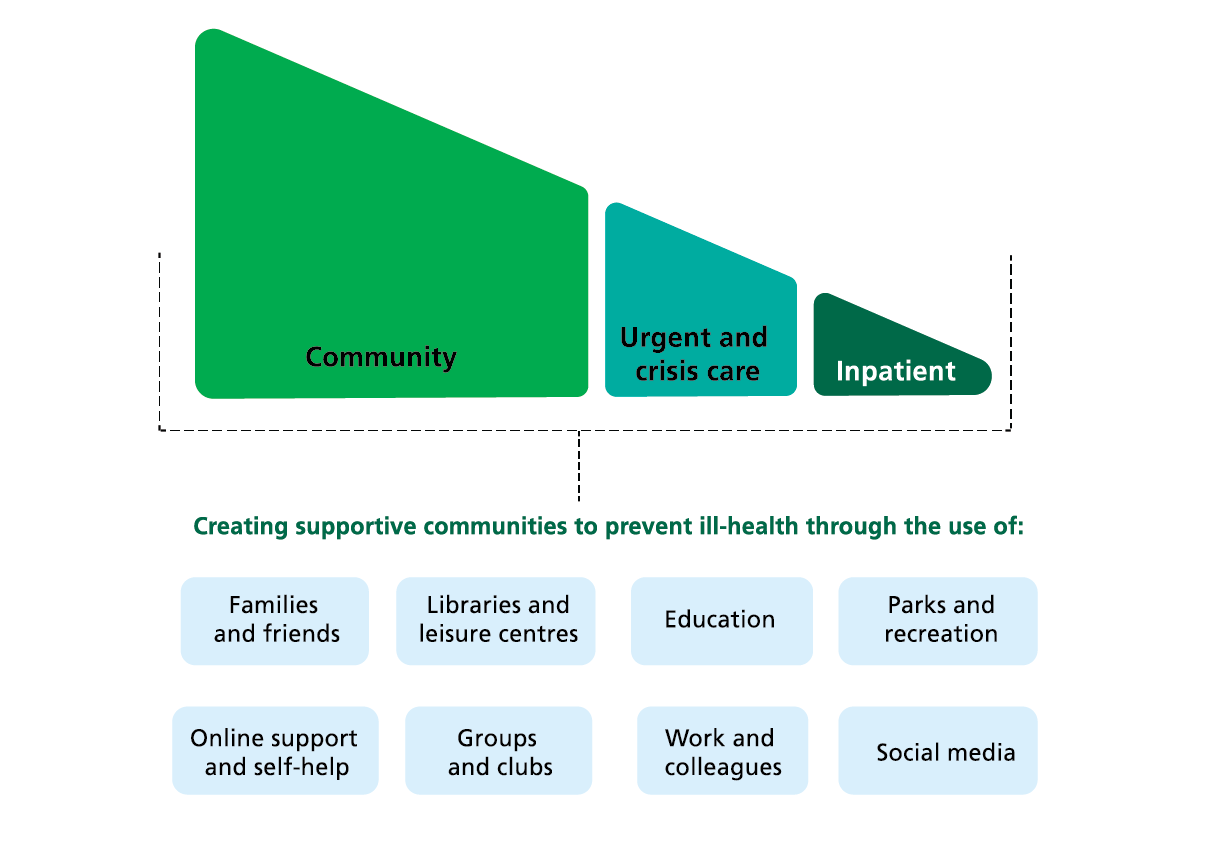
Creating supportive communities to prevent ill-health through the use of:
- Families and friends
- Libraries and leisure centres
- Education
- Parks and recreation
- Online support and self-help
- Groups and clubs
- Work and colleagues
- Social media
This strategy also applies this preventative and community-focussed approach to physical health. The priorities set out here aim to keep people well by providing them with the support, environment and access to services needed to prevent physical ill-health and to identify and address any physical health issues early.
We tend to see a higher proportion of male inpatients, particularly aged 30 – 50 years old. Amongst community/access service users, numbers were higher amongst under 18s and numbers of men and women are similar across all age groups (as seen in figure 4).
The majority of our service users in hospital (84%) and community/access services (85%) identify as White British.
Figure 4. CNTW service users by age and gender across inpatient and community/access settings
CNTW inpatient service users, by gender and age at year end 2024/25
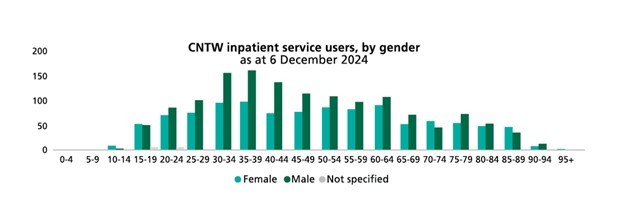
Service users are defined as a service user who has had one or more overnight stay during 2024/25.
CNTW community/access service users, by gender and age at year end
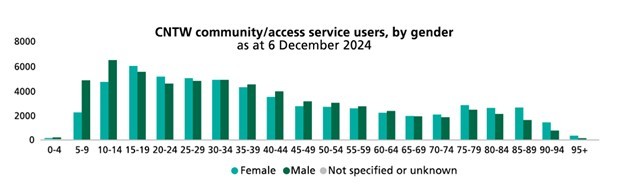
Service users are defined as a service user who has had one or more contact during 2024/25.
Figure 5 shows a breakdown of index of multiple deprivation (IMD) quintiles. The IMD is the official measure of how deprived an area is relative to the rest of England.
Deprivation is determined by looking at multiple factors including:
- Income
- Employment
- Barriers to housing and services
- Health deprivation and disability
- Education, skills and training
- Crime
- Living environment5
Quintiles are a way to present this data. The first quintile represents the most deprived 20% of the whole population of England, while the fifth quintile represents the least deprived 20%.
In figure 5 we can see that a far greater proportion of our service users in both inpatient and community settings live in the two most deprived quintiles than the two least deprived. This follows a trend that we see in many measures known as the ‘socio-economic gradient’, where people who live in areas of higher deprivation have worse health outcomes.
Put simply, our service users are more likely to live and work in areas of higher deprivation. Not only has this increased their risk of developing mental health illness, but it also means they are more likely to have physical health problems.
This means the need for prevention of physical illness and management of long-term physical health conditions in our service user population is high.
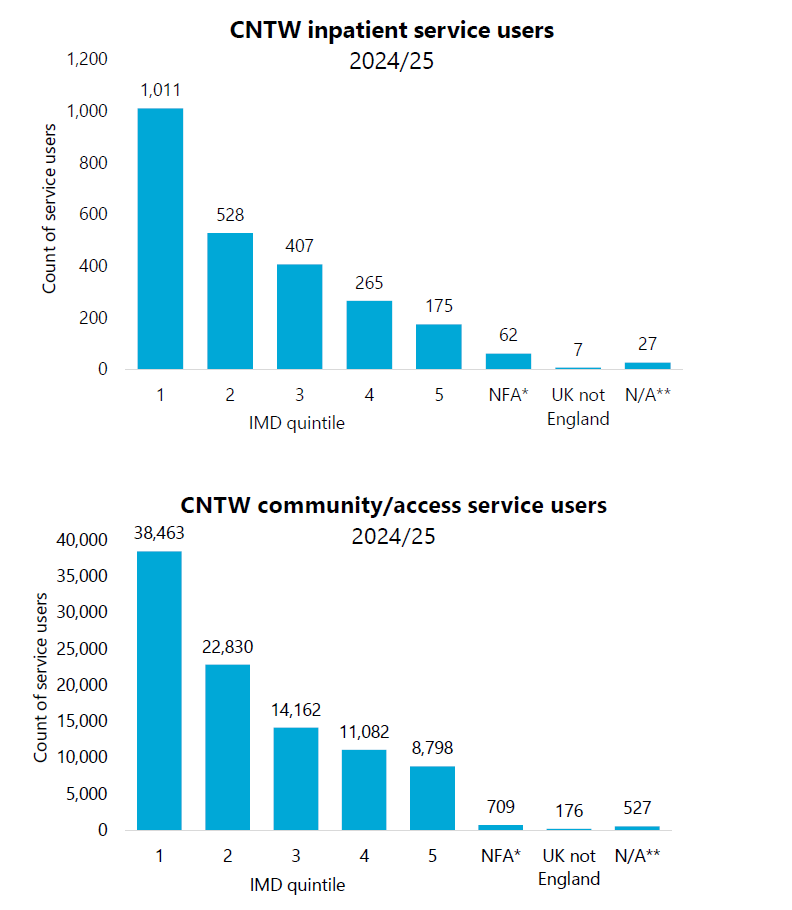
*NFA = No fixed abode. **N/A invalid postcode, unable to obtain IMD quintile.
1 = most deprived quintile, 5 = least deprived quintile.
CNTW inpatient service users are defined as a service user who has had one or more overnight stay during 2024/25.
CNTW community/access service users are defined as a service user who has had one or more contact.
We know that people with mental illness are more likely to experience:
- Poverty
- Homelessness
- Incarceration
- Social isolation
- Unemployment
These social inequalities can also have a significant impact on people’s ability to engage with physical health services and support, as they may not have the financial means to travel to appointments or take part in things such as exercise classes.
Employment
For those in contact with secondary mental health services, the employment rate was 67.4 percentage points lower than the overall rate.
Benefits
50.9% of Employment Support Allowance Claimants have a primary condition of a mental and behavioural problem.
Social isolation
Psychotic disorder is more common in people living alone. Evidence suggests links between mental illness, social isolation, and the challenges that people with psychotic disorder may face with maintaining relationships.
Housing
54% of adults (age 18-69) receiving secondary mental health services on the Care Programme Approach were recorded as living independently, with or without support.
Case study:
Supporting service users in the community
"My experience with the Scheme and the tobacco dependence advisor was really good. It was always in my mind to try and stop again at some point in the future, and being told about the offer of free vapes and vouchers (I am unemployed and do not have much money) motivated me to have a go.
Wayne gave me a lot of information, advice and encouragement along the way. I enjoyed using the CO monitor and Wayne explained the benefits of keeping the CO numbers low. Thank you for helping me quit."
As explained, our service users are already at a higher baseline risk of poor physical health than many others around the country. Life expectancy (how long you live) is lower in the North East and North Cumbria than nationally, with women and men both dying almost 2 years sooner than the national England average.
The differences in healthy life expectancy (how long you live in good health) are even greater: in some areas of the North East both women and men can have almost 6 years less of healthy life than the UK average.
In addition to this, people with serious mental illness (SMI) and those with learning disability face significant physical health inequalities compared to the general population. They:
Are more likely to have a chronic condition
People with SMI are more likely to experience conditions such as heart disease, diabetes, obesity, lung disease and cancer.1 They are almost two times more likely as a member of the general population to have diabetes, and more than twice as likely to have Chronic Obstructive Pulmonary Disease (COPD). People with learning disability are also more likely to have asthma, diabetes, heart disease or high blood pressure.
Are more likely to die at a younger age
Life expectancy for people with SMI is 15-20 years shorter than the general population, and around two thirds of premature deaths among adults with serious mental illness are from preventable physical illnesses. For people with learning disability on average men and women die 20 years and 23 years younger than the general population, respectively.
Are more likely to have unhealthy behaviours
Higher rates of smoking: people with SMI are more than 3 times as likely to smoke as the general population. Physical inactivity and poor nutrition are also more prevalent among people with SMI and learning disability, contributing to poorer physical health.
Experience greater barriers to accessing healthcare
Individuals with SMI and learning disability may face stigma, fragmented care, and challenges in accessing healthcare services, leading to late diagnoses and suboptimal management of physical health conditions.6 One example of this is cervical cancer screening rates, as in 2017/18 only a third (31%) of women with learning disability had cervical smear tests, compared to over two thirds (73.2%) of those without a learning disability.
May have physical side effects of medications
Psychotropic medications, especially antipsychotics, can increase the risk of weight gain, metabolic syndrome, and other physical health conditions.
Are more likely to be misdiagnosed due to ‘diagnostic overshadowing’
People with SMI and learning disability often experience diagnostic overshadowing, where healthcare professionals attribute physical symptoms to their mental illness or learning disability rather than investigating underlying physical health conditions. Alongside a lack of reasonable adjustments this can lead to delays or omissions in diagnosing and treating serious physical health issues, worsening health outcomes.
Are more likely to have poorer sexual health
Individuals with SMI and learning disability are more likely to have unsafe sex, putting them at an increased risk of sexually transmitted infections (STIs), unplanned pregnancies, and sexual dysfunction. Factors contributing to this
include lack of access to accessible sexual health education, stigma and access to and take-up of sexual health screening.
Are more likely to have poor oral health
People with SMI and learning disability are more likely to have poor oral health including untreated tooth decay and gum disease. Risk factors include high sugar intake, smoking and alcohol consumption, dry mouth as a side effect of medication, reliance on carers to engage with oral care or anxiety around visiting the dentist.
Poor oral health can have a significant impact including pain, restricted food choices and associations with other physical health conditions such as heart disease and stroke.
We see the issues above reflected in our own service user population. From 2019-2024 two main causes of death amongst our service users were cancer (12.6%), which can often be detected and treated by screening, and ischaemic heart disease (7.1%), which is highly preventable.25 In 2024 over a fifth (23%) of CNTW inpatients were smokers, compared to only 11% of the general population in the North East.26 Furthermore, almost a third (29%) had obesity.
As we’ve seen, people in our care are at higher risk of poor health and social outcomes. This can be further exacerbated if they are also part of other demographics that experience inequalities, such as being from the global majority* or LGBTQ+**, a concept known as ‘intersectionality’. It is therefore crucial for us to tackle these inequalities wherever we can.
Footer:
*A collective term for people of African, Asian, indigenous, Latin American, or mixed-heritage backgrounds
** Lesbian, Gay, Bisexual, Transgender, Queer or other identities like Intersex or Asexual.
Case study:
Supporting service users as inpatients
Occupational Therapy (OT) supported a female long stay patient (14 years as an inpatient), with a complex history of challenging behaviours who wished to be able to attend aqua fit.
OT staff spent months attending aqua fit sessions with her, slowly increasing her independence and confidence in travelling to sessions, engaging with classes and speaking to others there.
The skills and confidence she gained over this time has meant that moving to community accommodation has been made possible.
“Sharon built my confidence and self-esteem when I had none. She carried my hope when I had none, even in my darkest days.”
Case study:
Supporting our staff
"I received support from the quit team, and I found that Lisa was very down to earth which I felt that was very professional which helped me stop smoking.
I do feel confirmed that I am not going to start smoking again as I have been smoke free now for around 4 months which is a huge achievement."
At listening events held with service users and staff you told us:
- "My mental health and physical health needs are joined up and shouldn’t be treated as separate things".
- "I want to feel like a person and not just a number".
- "I don’t want to feel like medication is the default answer to everything".
- "It is frustrating to be sent between services and still not get the help I need. Seeking help and support should not feel like a fight with the system".
- "We hear generic terms like “eating better” but what does that actually mean?"
- "Physical healthcare shouldn’t be a ‘postcode lottery’".
We developed four core principles on the basis of what we heard. They were:
- Reducing health inequalities: Ensuring equitable access to and experience of physical health care for all service users, regardless of background or condition, as well as ensuring equitable outcomes of care for all service users.
- Joined up care: Delivering coordinated care at the right time and in the right place, integrating physical and mental health services seamlessly.
- Empowerment: Encouraging service users to take an active role in managing their own health, supported by education and resources.
- Culture: Embedding a culture of wellness across the trust, making every contact count
(MECC) to ensure interactions with our staff support both mental and physical health.
These core principles underline our ambitions moving forward, presented in line with current Trust strategic ambitions, to allow for joined-up working across the whole organisation.
We are also committed to addressing the physical health needs of our service users in line with the Core20PLUS5 framework.
This is a national NHS England approach to reducing healthcare inequalities at both national and system level. The approach defines a target population – the ‘Core20PLUS’ – and identifies ‘5’ focus clinical areas requiring accelerated improvement.
This approach has been adapted for healthcare inequalities experienced by both adults
and children and young people, as seen in the figures below.
View Core20PLUS5 approach for adults here.
View Core20PLUS5 approach for children and young people here.
Aligning with Trust ambitions
Based on insights from physical health data, staff and service users this strategy outlines the following key ambitions to improving our service users’ physical health:
We want to deliver expert, compassionate, person-led care in every team, every day.
We are dedicated to holistic, person-centred care that fully integrates physical and public health within mental health, learning disabilities, neuro disabilities and autism services. Recognising the critical link between physical and mental health, we want to ensure that our service users receive regular physical health checks and necessary follow-up, partnering with others to provide specialised care.
We strive to enhance both physical and mental health outcomes, helping people live safer, healthier lives, aspiring to make every contact count.
We will:
1.1 - Conduct regular assessments of service users’ physical health needs, ensuring appropriate follow-up through screening, interventions, and outcome monitoring.
1.2 - Identify and address differences in physical health outcomes within our service user population, recognising that many service users experience multiple layers of disadvantage due to their race, gender and mental health or learning disability diagnoses.
1.3 - Ensure a sustained increase in the number of Annual Health Checks for inpatients and community.
1.4 - Ensure every interaction with service users and carers enhances both physical and mental health, championing the Making Every Contact Count approach.
1.5 - Recognise when physical health needs require prompt escalation, using appropriate early warning scores (NEWS2/PEWS/MEOWS).
1.6 - Support health improvements through targeted interventions for smoking, alcohol, substance use, and obesity. We will educate and empower individuals to manage their health, promoting weight management and physical activity, and providing a healthy food environment for inpatient services.
1.7 - Maintain our hospitals as smoke free sites.
1.8 - Develop robust physical health liaison services involving medical consultants, senior registered nurses and other Allied Health Professionals (such as dieticians, occupational therapists, physiotherapists and speech and language therapists) to provide advice to support service users and staff in both community and inpatient settings.
1.9 - Work with acute trust partners to improve pathways for medical review, thereby reducing Emergency Department wait times when semi-elective admissions may be more appropriate.
1.10 - Engage with national work programmes such as STOMP (stopping over medication of people with a learning disability and autistic people) and STAMP (supporting treatment and appropriate medication in paediatrics) to prevent over-medication and reduce physical health impact of psychiatric medications.

We will work with partners and communities to support the changing needs of people over their whole
We are committed to delivering service user-centred care that respects and celebrates the individuality of each person. We strive to foster an inclusive, compassionate, and holistic approach that meets service users where they are, tailoring our care to their unique values, needs, and cultural backgrounds. Our aim is to create a supportive environment that prioritises realistic and adaptive care plans, promoting healing and wellness for all.
We will:
2.1 - Involve service users in their own care by actively listening to their needs, promoting self-responsibility, and empowering them to make informed decisions. This includes ensuring materials that help service users make decisions are in an accessible format.
2.2 - Recognise the essential role of family members and caregivers in supporting service users’ well-being by providing them with the education and resources they need to be effective allies in the healthcare process, in line with the six standards of our Triangle of Care accreditation.
2.3 - Identify and reduce barriers that limit access to community care such as poor transport links, language challenges, and geographical or sensory-access issues.
2.4 - Ensure clear and accessible pathways for the management of physical health conditions to support better care. This includes access to key physical health services such as screening, physiotherapy, podiatry, nutrition, oral health support and occupational therapy.
2.5 - Work with acute trust partners to improve the understanding and implementation of reasonable adjustments across care pathways, including utilising tools such as ‘hospital passports’.
We will make sure that our workforce has the right values, skills, diversity and experience to meet the
Our ambition is to prioritise staff well-being, empowering our teams to model and promote healthy behaviours while fostering a culture of holistic, high-quality care that integrates physical and mental health services.
We are committed to creating a supportive workplace where staff are trained
and equipped to address physical, public and mental health needs. By building a diverse workforce that values the knowledge and experiences of all team members, we aim to lead by example in delivering comprehensive, compassionate care.
We will:
3.1 - Strengthen our commitment to staff well-being by enhancing access to physical health support alongside mental health support. Ensure our staff policies promote a healthy working environment, serving as a positive example for service users.
3.2 - Implement and embed the Health Education England (HEE) Competency Framework for Physical Skills in a Mental Health and Learning Disability Setting and use this framework during annual appraisal for staff.
3.3 - Provide core physical health training, ensuring all frontline nurses and healthcare support staff complete essential training on physical health basics, monitoring, and health promotion. This includes providing access to training in specialist physical health skills required to support our service users.
We will ensure physical health training includes a trauma informed perspective, including an understanding of how Adverse Childhood Events (ACEs) can impact physical health and how to deliver physical health care from a trauma informed perspective.
3.4 - Develop shared training opportunities with acute trust partners to facilitate skills and knowledge sharing of key physical and mental health care concepts.
3.5 - Advocate for Allied Health Professionals and Mental Health Nurse training to include and optimise exposure to physical health settings, working with local partner universities and key clinicians within CNTW to do so.
3.6 - Support staff to become Physical Health Champions and see this role as integral to the mental health offer.
We will be a sustainable, high performing organisation, use our resources well and be digitally enabled.
We strive to be flexible and innovative in addressing ongoing challenges to physical health within our communities, while ensuring successful practices remain sustainable.
We recognise how important the health of the planet is for the physical and mental health of our service users and aim to make environmental sustainability a priority.
We will:
4.1 - Use our buildings and grounds as a resource for inpatient and community-based service users by allocating dedicated spaces for physical activity and ensuring they are fit for this purpose.
4.2 - Utilise technology to increase awareness of, and access to, physical health support, including signposting to other services.
4.3 - Make environmental sustainability a key element of how current and future services within our physical health offer are assessed, including in the process of commissioning.
We will create trusted, long-term partnerships that work together to help people and communities.
We believe that to build a robust and equitable physical health offer we cannot work alone. We aim to work with communities across the Trust (including service users, carers and staff) to ensure that services accurately reflect their needs.
We will also work with the public and wider partners to ensure everyone is able to access the physical health support they need, regardless of where they live.
We will:
5.1 - Develop a physical health offer that is of a consistent standard across localities, while accepting that resource may differ based on prevalence, demographics and geography. This will remove the risk that our physical health offer is a ‘postcode lottery’.
5.2 - Ensure the physical health offer has parity across the Trust footprint and that a service users’ physical health and wellbeing isn’t seen as secondary to their mental health.
5.3 - Work as a system in partnership with primary and secondary care, local authorities and voluntary, community and social enterprise (VCSE) organisations to provide a robust and equitable physical health offer.
5.4 - Include commissioning in discussions around transformational change, allowing commissioners to understand the rationale behind new services or changes to services that they would be funding. This aims to make services more inclusive and meet the needs of the population where the service would be changed.
How will we know we have succeeded?
This strategy has established our vision for creating a service that enables all those in our care to become and remain physically healthy, including ambitions that detail how we plan to meet this aim.
We have also developed a guiding framework that includes key outcomes and signs of progress and which will be monitored through Public and Physical Health Steering Group. This will be circulated internally and will be regularly updated to see when we are on the right track and when our approach might need adjusting.
Conclusion
This strategy aims to be ambitious and aspirational in tackling the disparities we see in physical health outcomes between people with a serious mental illness or learning disability and the general population. We believe that supporting our service users to become and remain physically healthy is a core part of our mental health offer.
At CNTW, physical health is everyone’s business. We will achieve improved outcomes by using the tools and spaces already at our disposal, by utilising and further developing the skills and knowledge amongst our staff, by continuing to work closely with our service users as well as their carers and families, and by building strong and lasting partnerships with healthcare and community partners.
Most importantly, this strategy takes a proactive approach to physical health that prevents the development of physical illness and treats and manages conditions early. It highlights the importance of identifying and addressing where access to and experience of care is different within our service user population and sets out ways in which we can address these inequalities.
By doing so, we will ensure that everyone in our care is supported as a whole person with both mental and physical health needs, no matter who they are or where they live.